
Vestibular neuritis radiology-various-aspects-
Vestibular neuritis, often referred to as acute unilateral vestibulopathy (AUVP) or vestibular neuronitis, is identified as presumed inflammation of the vestibular nerve or vestibulocochlear nerve. It may be linked with labyrinthitis.
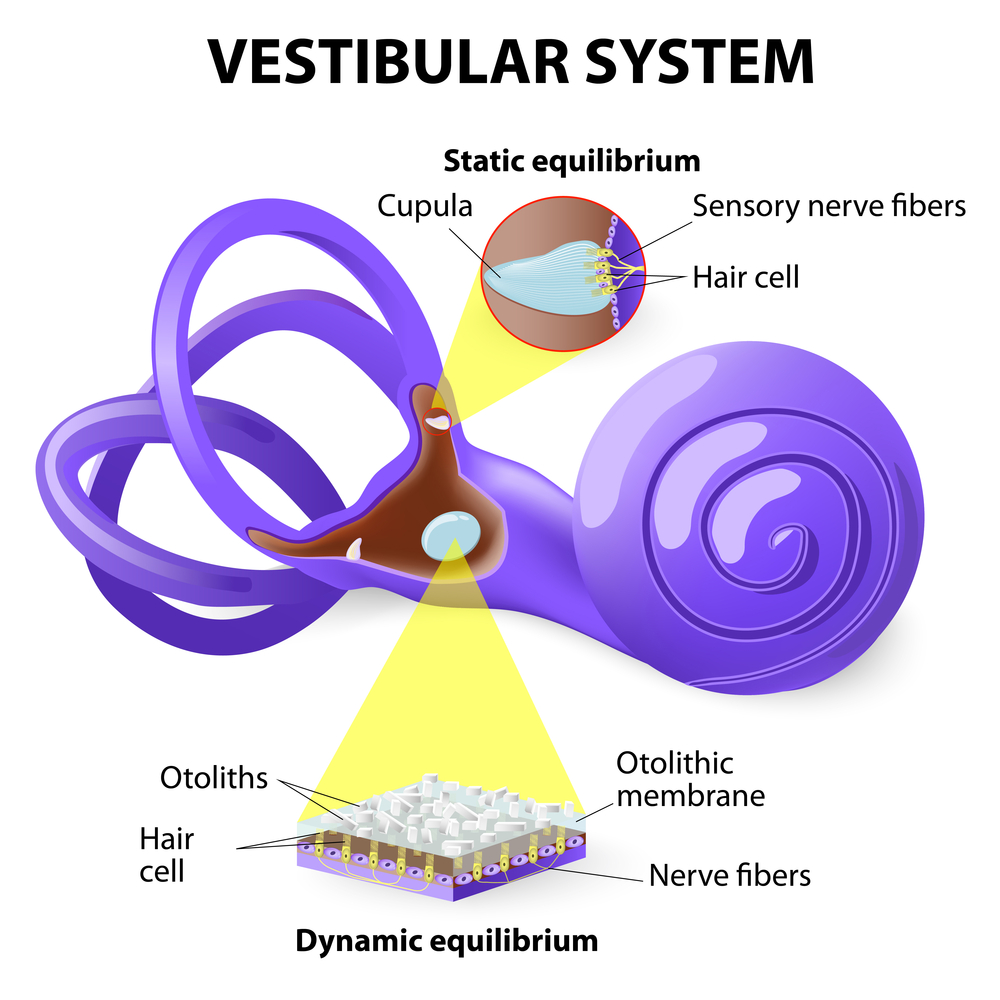
The vestibular nerve is a significant branch of cranial nerve eight (CN VIII) that conveys equilibrium signals from the inner ear to the central nervous system. The cochlear nerve represents the other major branch of the vestibulocochlear nerve that carries auditory information to the central nervous system. Inflammation of the vestibular branch of CN VIII (vestibulitis) is associated with symptoms of vertigo.
Conversely, the swelling of both the vestibular and cochlear nerve bundles (labyrinthitis) also causes tinnitus and/or hearing issues in addition to vertigo.
If any patient of ENT requires any surgery, opd consultation or online consultation in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may contact him at the following address-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road, Ambad ,1 km from Pathardi phata Nashik ,422010, Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cell no- 7387590194 , 9892596635
Issued in public interest by –

Epidemiology
Some regard this as the third most frequent cause of peripheral vestibular vertigo. An estimated annual incidence is 3. 5 per 100,000 individuals and may represent 7% of patients in outpatient clinics focused on treating vertigo. Vestibular neuritis is prevalent among both men and women aged 30-60 years old.
Clinical presentation
Certain patients may report a preceding gastrointestinal or upper respiratory tract infection history, especially among individuals aged 30-60 years.
Otherwise, the syndrome typically presents with:
– vertigo, sudden and severe
– spontaneous horizontal nystagmus, where the fast phase beats away from the affected side (according to Alexander’s law)
– balance/gait difficulties
– nausea and vomiting
– concentration issues
After symptom recovery, balance and dizziness disorders may persist for several months in some patients.
For update on further important health related topics and frequently asked questions on health topics by general population please click on the link given below to join our WhatsApp group –
https://chat.whatsapp.com/Lv3NbcguOBS5ow6X9DpMMA
Issued in public interest by –
Pathology
Typically, the superior division of the vestibular nerve is impacted, resulting in the involvement of the superior and horizontal semicircular canals; however, both divisions may also be simultaneously affected. Viral infections are believed to be the most common causes of vestibular neuritis, with bacterial infections occurring much less frequently. The most frequent viral causes of vestibular neuritis include herpes simplex virus (HSV-1) (considered the most common viral etiology), measles, rubella, mumps, Epstein-Barr virus, influenza, and varicella/herpes zoster.
Radiographic features
MRI
MRI with contrast is occasionally requested to rule out other reasons for sudden onset dizziness and vertigo, such as stroke (particularly AICA territory strokes) and brain tumors, especially in older patients. However, the MRI findings are typically normal in cases of vestibular neuritis.
T1 C+ (Gd): may reveal enhancement of the vestibular nerve fibers within the internal auditory canal, while the labyrinth of the inner ear is usually intact.
Treatment and prognosis
Corticosteroids, antiemetics, and vestibular physiotherapy are standard supportive care measures. Antiviral or antibacterial treatments are generally unnecessary. Recurrence is infrequent, and most patients will achieve full recovery.
Differential diagnosis
- – AICA territory ischemic stroke
- – isolated nodular ischemic stroke
- – anti-GQ1b antibody syndrome
Issued in public interest by –


