
Ear canal wall up mastoid surgery-various aspects-
A canal wall up mastoidectomy is a surgical operation that eliminates infected bone from the mastoid area while preserving the ear canal. It is one of the primary forms of mastoidectomy procedures.
A canal-wall-up mastoidectomy is a surgical technique that retains the external auditory canal while eliminating the mastoid air cells. It is also referred to as a tympanomastoidectomy or intact-canal wall (ICW) mastoidectomy.
If any patient of ENT requires any surgery, opd consultation or online consultation in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may contact him at the following address-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road ,Ambad ,1 km from Pathardi phata Nashik ,422010 ,Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cel no- 7387590194 , 9892596635
What it’s used for Treating acute mastoiditis and Managing chronic ear disease.
How it’s performed
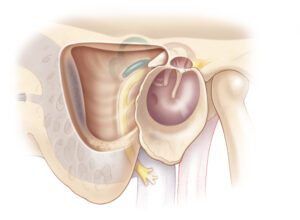
An “ear canal wall up mastoid surgery,” also referred to as a “canal wall up mastoidectomy,” entails gaining access to the mastoid bone situated behind the ear via an incision, eliminating infected air cells within the mastoid while maintaining the posterior wall of the ear canal (the canal wall), and subsequently reconstructing the surgical area by keeping the canal wall intact, essentially “up” in its original alignment; this procedure is generally conducted under general anesthesia to extract cholesteatoma or address chronic ear infections that have extended to the mastoid bone.
A canal wall up mastoidectomy, or tympanomastoidectomy, retains the posterior bony wall of the external auditory canal during the procedure to reach the mastoid cavity, whereas a canal wall down mastoidectomy removes this wall, resulting in a larger, open cavity.
Canal Wall Up Mastoidectomy:
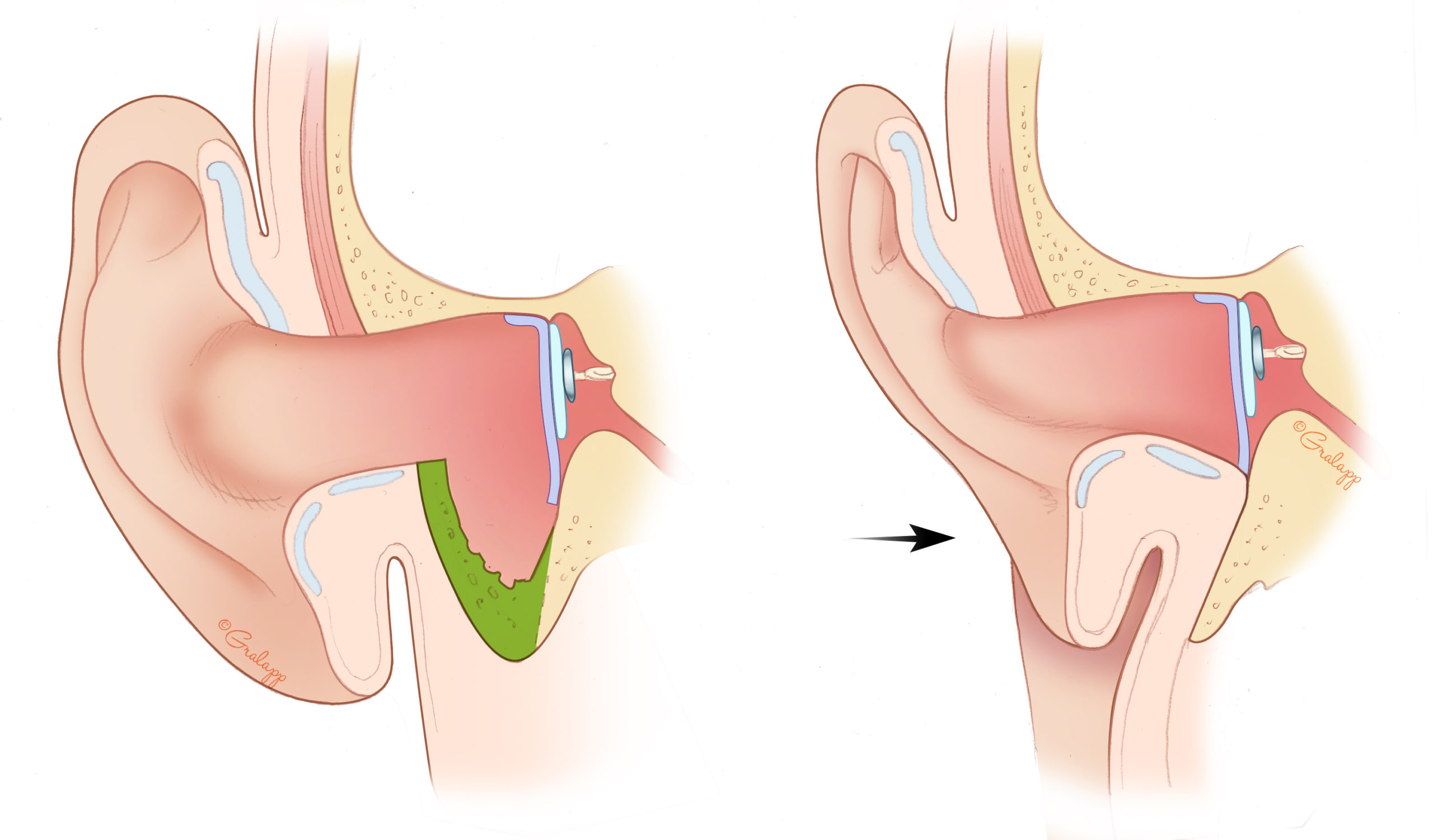
- This procedure seeks to maintain the posterior bony wall of the ear canal (the wall separating the ear canal from the mastoid cavity).
- It’s generally employed for initial instances of acute mastoiditis or for situations where the disease is constrained and the ear canal remains intact.
- The surgeon accesses the middle ear space (behind the eardrum) and the mastoid cavity by excising the mastoid air cells, while preserving the canal wall.
- This method intends to maintain the natural anatomy of the ear canal and middle ear.
For Update On Further Important Health Related Topics And Frequently Asked Questions On Health Topics By General Population Please Click On The Link Given Below To Join Our WhatsApp Group –
https://chat.whatsapp.com/Lv3NbcguOBS5ow6X9DpMMA
Key steps of a canal wall up mastoidectomy:
Incision:
The surgeon creates a post-auricular incision behind the ear to reach the mastoid bone.
Bone removal:
Utilizing specialized instruments such as a drill, the surgeon carefully extracts the mastoid air cells, exposing the mastoid antrum (the central cavity of the mastoid) while safeguarding the posterior wall of the ear canal.
Facial nerve identification:
Throughout the surgery, the surgeon must diligently recognize and avoid harming the facial nerve, which is positioned near the mastoid cavity.
Cholesteatoma removal:
If the operation is intended for cholesteatoma, the surgeon will carefully eliminate all remnants of the cholesteatoma tissue from the middle ear and mastoid cavity.
Closure:
Once the requisite bone is removed and the affected area is cleansed, the surgical site is secured with sutures, and a dressing is applied.
Canal Wall Down Mastoidectomy:
- This procedure entails removing the posterior bony wall of the ear canal, resulting in a large, open cavity that unites the ear canal, mastoid, and middle ear spaces.
- It’s usually reserved for instances of chronic otitis media, recurrent cholesteatoma, or when the ear canal is significantly damaged or infected.
- The opening of the ear canal is often expanded to enhance cleaning and access to the mastoid cavity.
- This technique is sometimes referred to as a radical or modified mastoidectomy.
Important considerations:
Canal wall down vs. canal wall up:
A “canal wall down” mastoidectomy involves excising part of the posterior ear canal wall as well, which may be essential in specific circumstances where access to the middle ear is required.
Postoperative care:
After surgery, patients will generally need to manage pain with medication, maintain cleanliness of the surgical site, and refrain from water exposure for a designated timeframe.
- The surgeon excises more bone than in a simple mastoidectomy to reach the middle ear space.
- The surgeon removes Koerner’s septum to form a mastoid bowl that connects with the antrum and epitympanum.
- The surgeon repairs any canal defects using cartilage or bone grafts.
Comparison to canal-wall-down mastoidectomy
A “canal wall up” mastoidectomy retains the posterior wall of the ear canal, maintaining the mastoid cavity’s separation from the ear canal, whereas a “canal wall down” mastoidectomy eliminates this wall, effectively forming a single open space between the mastoid and ear canal; the principal distinction centers on whether the bony barrier separating the ear canal and mastoid is preserved during the operation, with “canal wall up” retaining it and “canal wall down” discarding it, influencing accessibility for post-operative evaluation and the recurrence risk based on the condition treated.
DISCLAIMER-Some patients go to net and directly take treatment from there which can lead to catastrophic consequences-Then- Many people ask then why to read all this text -the reason is that it helps you to understand the pathology better ,you can cooperate with treatment better ,your treating physician is already busy with his patients and he does not have sufficient time to explain you all the things right from ABCD ,so it is always better to have some knowledge of the disease /disorder you are suffering from.
Key points to consider:
Access and monitoring: A canal wall down surgery affords enhanced access to the mastoid cavity for thorough disease excision, but necessitates more vigilant post-operative management due to the open cavity, while a canal wall up procedure might render certain areas more challenging to observe for potential recurrence.
Cholesteatoma management: For cholesteatoma treatment, a canal wall down technique is frequently favored as it permits a more complete excision of the lesion, while a canal wall up approach could be applied for smaller or less invasive situations where it is essential to preserve the ear canal anatomy.
Hearing preservation:
Canal wall up techniques typically provide superior hearing preservation in comparison to canal wall down procedures, as they minimally disturb the middle ear components.
Patient management:
Canal wall down surgery often necessitates more regular post-operative cleanings and stringent water restrictions due to the open cavity, whereas canal wall up may involve less rigorous post-operative maintenance.
When to choose each procedure: Canal wall up:
Smaller cholesteatoma Desire for enhanced hearing preservation Cases where retaining ear canal anatomy is vital
Canal wall down:
Large or extensive cholesteatoma High probability of recurrence with canal wall up method Situations needing ample exposure for total disease excision
- A canal-wall-down mastoidectomy removes the posterior and superior walls of the external auditory canal.
- A canal-wall-down mastoidectomy is typically designated for patients with chronic otitis media or recurrent cholesteatoma.
Other names Tympanomastoidectomy, Intact-canal wall (ICW) mastoidectomy, and Combined approach.
Canal wall up and down mastoidectomy
Canal wall up (CWU) and canal wall down (CWD) mastoidectomies are operations that provide access to the middle ear. The primary distinction between the two lies in the preservation of the ear canal.
Like a canal wall up mastoidectomy, it involves the removal of the lateral wall of the mastoid, and Koerner’s septum is excised to establish a connection with the middle ear cavity 1. The key difference is that the posterior superior wall of the external acoustic meatus is also extracted 1.
The objective of cholesteatoma treatment is to eliminate the disease and establish a secure and dry ear while preventing the reappearance of the condition and preserving or potentially enhancing hearing (1). The optimal surgical technique for cholesteatoma treatment has been a topic of debate for many years. Although both canal wall down (CWD) and canal wall up (CWU) tympanomastoidectomy possess their pros and cons, the CWU method is frequently favored as it avoids the creation of a radical cavity. A radical cavity may lead to a situation with higher frequencies of recurrent otitis and necessitates consistent debridement. In contrast, the CWU method preserves the typical anatomy of the external ear canal, generally resulting in fewer instances of refractory otitis. Furthermore, after CWU surgery, routine debridement of the ear is typically not necessary, and hearing aids are better suited and more comfortably tolerated (2–4). However, a major concern linked to choosing the CWU method is the heightened risk of recurrent and residual cholesteatoma (5). In previous studies, recidivism rates—including both recurrent and residual rates—have been documented as 4 to 17% when employing CWD tympanomastoidectomy, compared to rates ranging from 9% to 70% with the CWU method (5, 6). Since the wide variation in prevalence cannot solely be attributed to the surgical method, various other factors must play a role, including the surgeon’s experience and patient-related considerations.
There has been increasing interest in filling the epitympanic and mastoid regions following either CWD or CWU tympanomastoidectomy, with the main aim of enhancing disease control. The initial efforts were recorded in 1911 by Mosher (7). Mercke was among the first otologists to report results with low recurrent and residual rates following obliteration in conjunction with CWD tympanomastoidectomy (8). Encouraging results as detailed by Offeciers et al. ensued using a different technique, which maintained the posterior canal wall (9). Recently, van der Toom et al. demonstrated in their systematic review that obliterating the mastoid decreases the recurrence rates for both the CWD (5. 9% recurrent rate, 5. 8% residual rate) and CWU techniques (0. 28% recurrent rate, 4. 2% residual rate) (6). Therefore, merging the CWU technique with obliteration appears to be a promising strategy to enhance disease control.
Issued In Public Interest By –
What is canal wall up mastoidectomy?
A canal wall up mastoidectomy is a surgical operation that excises bone from the mastoid bone while maintaining the posterior wall of the external auditory canal. This operation is utilized to address mastoiditis and cholesteatoma.
What it does
- Enables the surgeon to reach the middle ear space located behind the eardrum
- Forms a mastoid bowl or cavity
- Links the mastoid cavity with the antrum and epitympanum
When it’s performed
- Generally for the initial episode of acute mastoiditis
- May also be employed to manage cholesteatoma
Comparison to canal wall down mastoidectomy
- A canal wall down mastoidectomy removes the posterior and superior osseous external auditory canal
- A canal wall down mastoidectomy necessitates more regular mastoid cleaning appointments
Other considerations
- The type of mastoidectomy conducted relies on various factors, which include the patient’s anatomy, extent of disease, and risks to hearing and balance
- A canal wall up mastoidectomy can aid in preserving hearing and the structure of the ear canal
Is mastoid surgery serious?
Is mastoidectomy considered a major surgery? Mastoidectomy is indeed a major surgery. An individual will be given general anesthesia and may need as long as 12 weeks to completely recover.
-FOR FURTHER INFORMATION IN GREAT DETAIL ON Mastoid surgery complications PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION
-FOR FURTHER INFORMATION IN GREAT DETAIL ON Mastoiditis surgery cost in India PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
-FOR FURTHER INFORMATION IN GREAT DETAIL ON Mastoid surgery recovery PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
-FOR FURTHER INFORMATION IN GREAT DETAIL ON Mastoid surgery aftercare PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
-FOR FURTHER INFORMATION IN GREAT DETAIL ON Mastoidectomy Surgery: Benefits, Risks, and Recovery PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
Mastoid surgery, especially a mastoidectomy, is a procedure performed to remove diseased tissue, usually infected air cells, from the mastoid bone, which is situated behind the ear. This procedure is commonly performed to treat mastoiditis, cholesteatoma, or as a component of other operations, such as cochlear implantation.
The following is a more thorough explanation:
Goal:
The goal of a mastoidectomy is to eradicate infection and illness inside the mastoid bone, thereby preventing additional problems and the possibility of hearing loss.
Symptoms:
Mastoidectomy is frequently used to treat mastoiditis (an infection of the mastoid bone), cholesteatoma (a skin-lined cyst in the middle ear), and to gain access to the middle ear for other surgeries.
Method:
- An ENT surgeon usually does the surgery while the patient is under general anesthesia.
- To reach the mastoid bone, an incision is made behind the ear.
- To clear the area and remove the infected air cells, the surgeon employs a microscope and specialized equipment.
- After that, the wound is sutured shut, and a bandage is put on.
Different kinds of mastoidectomy:
- Basic Mastoidectomy: Entails removing the sick tissue while maintaining the ear canal wall.
- Radical mastoidectomy: Entails bringing the middle ear and mastoid outside by removing the ear canal wall.
Recovery:
Patients may experience some discomfort, disorientation, and transient hearing loss following surgery. Gauze can be used to pack the ear, and follow-up appointments are required to check the healing process and remove the packing.
Possible consequences:
Although uncommon, possible consequences include facial nerve injury, tinnitus, vertigo, and hearing loss.
How does the ear function?
The outer, middle, and inner ear make up the ear. The eardrum vibrates as sound travels through the outer ear. The vibration is carried via the middle ear’s three minute bones: the malleus, incus, and stapes. The inner ear is then invaded by the vibration, which causes nerve cells to generate signals that are sent to the brain and decoded as sound.
The balance mechanism, which is located in the ear, is made up of hairlike sensors and fluid-filled semicircular canals that aid in maintaining balance. The ear is the path through which the nerve that controls the muscles of the face passes. The brain is located right above the ear.
What is the mastoid bone?
Just behind the ear, one may feel the mastoid bone, which is a noticeable bony region. It connects to the air space in the middle ear and has a lot of air gaps. Middle ear disorders can spread into the mastoid bone.
What is the purpose of mastoid surgery?
Cholesteatoma is the ailment that accounts for the majority of mastoid operations. This is a cluster of dead skin cells that develops in the shape of a bag from the eardrum into the mastoid bone and middle ear. In some cases, mastoid surgery is done to give access for other procedures, like cochlear implant surgery.
What issues might result from cholesteatoma?
Recurring ear infections can result from the gradual growth of this skin sac over several years. The sac can also begin to gradually wear down the neighboring tissues in and around the middle ear as it grows. These are the tiny bones that send vibrations to the inner ear, the bony covering of the inner ear, the bone that protects the facial nerve, and the bone that lies between the ear and the brain.
What signs might I experience?
Recurrent ear infections might result in ear pain and a foul-smelling discharge. Hearing loss can be caused by the deterioration of ear structures. You could experience tinnitus, which is a sound in your ear like humming, hissing, or ringing, and your balance might be thrown off. On rare occasions, the illness might result in consequences like abscesses and meningitis. Fever, excruciating pain and swelling around the ear, and a stiff neck are other symptoms of this illness.
Do I require any testing?
Using a portable instrument called an otoscope, which has a magnifying lens and a light, your advisor will check your ear. They can utilize a suction device to extract any earwax and a microscope to get a closer look at your ear. This is quite secure, however it can occasionally result in minor pain and vertigo. An audiogram will be used to assess your hearing range. Your consultant may also recommend that you undergo an MRI or CT scan.
What kind of treatment might I require?
Your symptoms will only be relieved temporarily by ear suction and antibiotic treatment.
Surgery is the only treatment for cholesteatoma that is both safe and successful.
What are the advantages of having surgery?
The primary advantage of eliminating cholesteatoma is preventing ear infections. It can also help prevent potential problems that might occur if the cholesteatoma expands.
What happens during an operation?
The name of the procedure is also mastoidectomy. The size of the cholesteatoma frequently dictates the kind of mastoidectomy performed. Combined-approach tympanoplasty, atticotomy, and atticoantrostomy are some of the other names for this procedure.
General anesthesia is used in almost all procedures. It can take between one and three hours.
Your ear canal will be cut above or behind your ear. Some surgeons may perform the procedure via the ear canal if the illness is localized, using a form of telescope known as an endoscope to guide them. Sometimes, in order to access the condition, surgeons will utilize a drill to cut through the mastoid bone. In certain instances, a laser and an endoscope are used together with other combination methods.
After the bone that covers the infection inside the mastoid cells is removed, the area is left with what is known as a mastoid cavity. Some surgeons leave the mastoid cavity open to the ear canal. Others shut the mastoid cavity using bone, cartilage, or muscle taken from the area around the ear. This makes it simple for them to examine the mastoid cavity. To facilitate the examination and cleaning of the ear in the outpatient clinic, the aperture of the ear is occasionally enlarged. You should talk to your surgeon about which strategy you and them would prefer. Following surgery, packing will be inserted into your ear. Before being taken at a clinic, the packing may stay in place for up to three weeks as your ear recovers. Packing that does not require removal is used by certain surgeons. After seven to ten days, any stitches can be taken out at your GP office. It’s possible that you’ll also require a head bandage for as long as 24 hours.
Are there any options to surgery?
Surgery might not be the ideal solution for you in some cases. With your surgeon, you will make this choice. Regularly having your ear cleaned with suction at an ear, nose, and throat clinic and using antibiotic drops as needed may prevent the illness from spreading, but it will never be completely eradicated. The possibility that the cholesteatoma may grow and cause problems still exists. Among these uncommon side effects are meningitis, brain abscess, facial paralysis, vertigo, and complete hearing loss.
What can I anticipate after the surgery?
You will be taken to the recovery room after the procedure. You’ll be brought back to the ear, nose, and throat ward after your anesthesia wears off. You might wear a bandage over your head and a dressing over your ear.
Following the surgery, your ear will hurt, and you’ll be given painkillers both during your hospital stay and to bring home with you. The pain from this can last for as long as two weeks. For as long as three weeks, you’ll be thinking about packing, which will make your ear feel blocked. Due to the packing or your wound, you may experience a little bleeding. Cotton wool and a bandage can be used until the bleeding stops, but keep in mind that these should be changed frequently. The practice nurse at your GP will remove the stitches between seven and fourteen days later. If the contents of your luggage start to fall out, you may cut off the loose end with a pair of clean scissors while leaving the remainder in place. You should keep your ear dry for as long as your surgeon recommends.
Contact the ear, nose, and throat department of your neighborhood hospital if you have any worries regarding your ear.
How long will my hospital stay be?
Although you might be able to return home the same day, be ready to spend the night in the hospital. Following surgery, you may require a longer hospital stay if there are any complications.
How long does it take to recover?
The speed of your recovery depends on the scale of your business. After two weeks, you might be able to return to work, but you’ll need to keep your ear dry. After six to eight weeks, the majority of individuals will have made a complete recovery.
Post-treatment care
A few weeks after surgery, you’ll need an outpatient appointment at the hospital. If you have packing in your ear, it will be taken out during this visit. Following mastoid surgery, it is typical to require extensive follow-up treatment, particularly if you have a mastoid cavity.
If any patient has any ENT -Ear nose throat problems and requires any , consultation ,online consultation ,or surgery in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may TAKE APPOINTMENT BY CLICKING ON THE LINK GIVEN BELOW-
Clinic address of ENT SPECIALIST doctor Dr Sagar Rajkuwar-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road ,Ambad ,1 km from Pathardi phata Nashik ,422010 ,Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cel no- 7387590194 , 9892596635


