
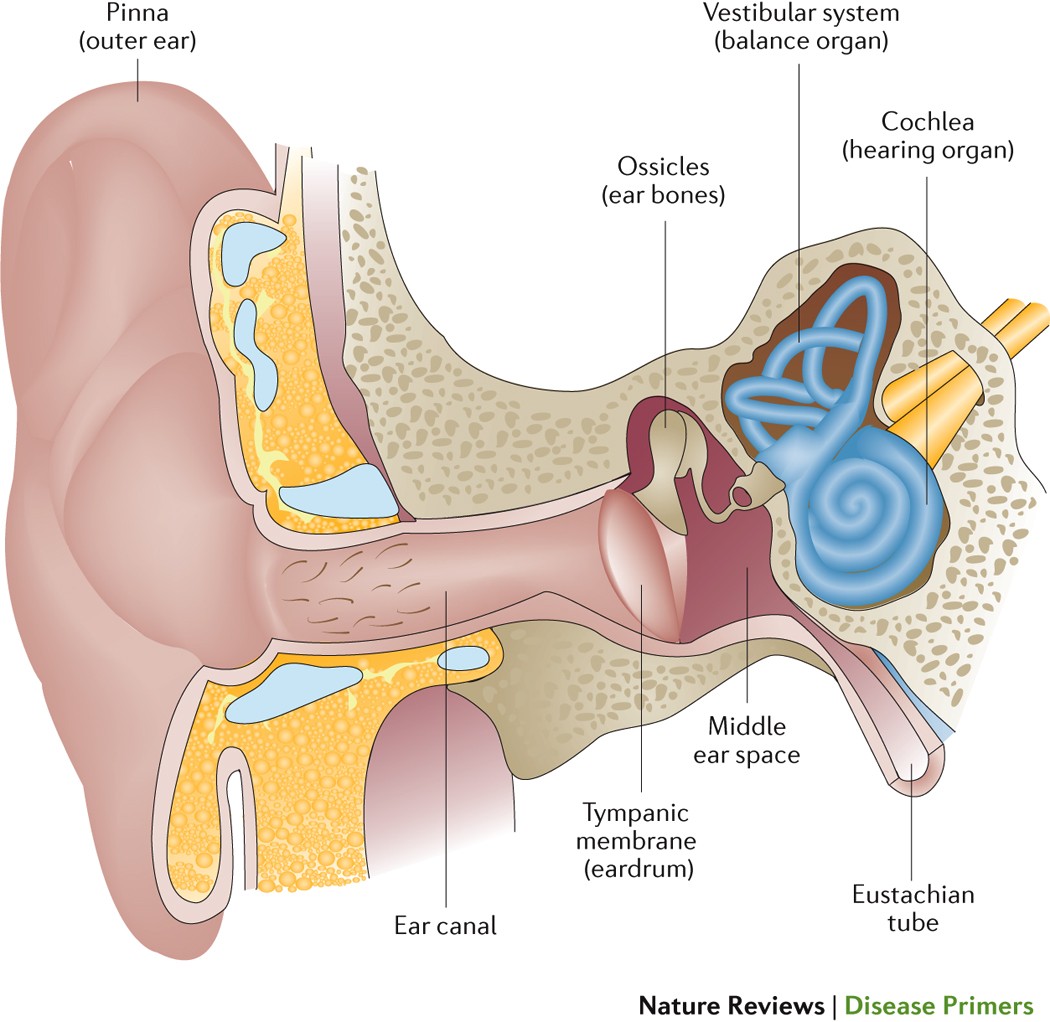
Chronic Otitis Media Effusion-various aspects- Chronic Otitis Media Effusion-Otitis medium with effusion (OME) is a condition in which the middle ear is filled with fluid but does not exhibit acute infection symptoms. The tympanic membrane is pressed against as middle ear and Eustachian tube fluid accumulates. The pressure reduces sound conduction, which in turn reduces hearing by preventing the tympanic membrane from vibrating properly. The management of otitis media with effusion is reviewed, along with its aetiology and symptoms, in this activity, which also emphasises the importance of the interprofessional team.

Objectives for study of Chronic Otitis Media Effusion-
List the danger signs of otitis media with effusion.
Describe the patient’s presentation for otitis media with effusion.
Provide a brief summary of the otitis media with effusion treatment options.
Examine the significance of bettering interprofessional team member care coordination to enhance patient outcomes for those suffering from otitis media with effusion.
INTRODUCTION of Chronic Otitis Media Effusion
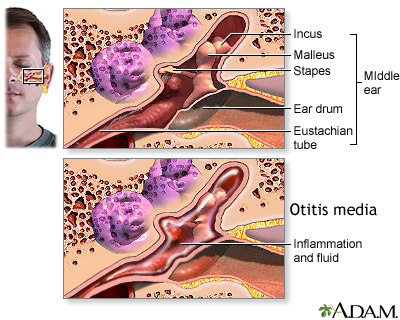
Otitis medium with effusion (OME) is a condition in which the middle ear is filled with fluid but does not exhibit acute infection symptoms. The tympanic membrane is pressed against as middle ear and Eustachian tube fluid accumulates. The pressure reduces sound conduction, inhibits the tympanic membrane from vibrating properly, and thus impairs patient hearing. Although some clinicians advise saving the term “chronic otitis media” for patients in whom the tympanic membrane has perforated, chronic OME is defined as OME that continues for 3 months or more on examination or tympanometry.
If Any Patient of ENT Requires Any Surgery, Opd Consultation Or Online Consultation In Clinic of ENT Specialist Doctor Dr. Sagar Rajkuwar ,He May Contact Him At The Following Address-
Prabha ENT Clinic, Plot no 345,Saigram Colony, Opposite Indoline Furniture Ambad Link Road ,Ambad ,1 km From Pathardi Phata Nashik ,422010 ,Maharashtra, India-Dr. Sagar Rajkuwar (MS-ENT), Cell No- 7387590194, 9892596635
Passive smoking, bottle feeding, daycare nurseries, and atopy are risk factors for OME. OME can affect both children and adults. These populations’ aetiologies, however, varied. The Eustachian tube is positioned more horizontally in younger children. The tube lengthens and angles caudally as the youngster grows into an adult. As a result, OME is more prevalent in youngsters, and at this age, the position of the head might affect how OME develops. [ Children who have abnormalities in the development of the palate, palate muscles, lower muscle tone for the palate muscles, or differences in the development of the bones are more likely to have OME, such as cleft palate and Down syndrome. In addition to these physical changes, individuals with Down syndrome may have problems with mucociliary function, which raises the risk of OME.
Epidemiology of Chronic Otitis Media Effusion
The most common cause of juvenile acquired hearing loss is OME, one of the most common infectious infections in kids. Children between the ages of 1 and 6 are most frequently affected by the illness. By age 2, the prevalence is higher; after age 5, it decreases. OME is more common in the winter, when patients are more likely to contract upper respiratory infections.
Pathophysiology of Chronic Otitis Media Effusion
Children who have an acute otitis media experience fluid accumulation in the middle ear, which prevents sound from reaching the inner ear by impairing vibration of the tympanic membrane. Children that have this impairment could find it harder to communicate in noisy settings. The youngster may display indicators of inattentiveness or poorer academic progress.
For Update On Further Important Health Related Topics And Frequently Asked Questions On Health Topics By General Population Please Click On The Link Given Below To Join Our WhatsApp Group –
https://chat.whatsapp.com/Lv3NbcguOBS5ow6X9DpMMA
Large adenoids can clog the Eustachian tube in individuals, which leaves the middle ear inadequately ventilated. OME could be brought on by this kind of obstruction. As a lymphatic structure, the adenoids may be able to spread germs into the Eustachian tube and promote the development of biofilms. As a result of such bacterial development, the middle ear may become inflamed, which could lead to blockage and fluid accumulation.
Histopathology of Chronic Otitis Media Effusion
The mucociliary defence system in the Eustachian tube is assumed to be the first line of defence in the middle ear. This defence system is aided by the mucosa’s production of immunoglobulins. These defensive systems might be overactive in OME as a result of the immunoglobulin levels being significantly elevated in effusions.
Toxicokinetics of Chronic Otitis Media Effusion
Otitis may also be brought on by viral or allergic-induced inflammation. While clinical practise guidelines found that there was insufficient evidence to support particular therapy options for allergy-induced OME, allergies are a substantial risk factor for otitis media. Nonetheless, it makes sense to draw the conclusion that vigorous therapy of allergic rhinitis might help individuals who also experience OME.
Physical and historical –Chronic Otitis Media Effusion
The most typical complaint among OME patients is hearing loss, albeit it is not always present. Patients and their parents may lament poor communication, disengagement, and inattentiveness. A physician may identify impaired speech and language development during an examination. These patients may experience intermittent otalgia and earaches. They frequently experience auditory fullness or the sense that their ears are popping. OME is more frequently unilateral in adulthood. Tinnitus and the impression of a foreign body in the external auditory canal have both been reported by adult patients. Chronic Otitis Media Effusion frequently arises in conjunction with upper respiratory infections in both infants and adults. As a result, it is essential to inquire about previous or recurring upper respiratory tract infections, nasal blockage, and ear infections from patients.
Physical examination findings for include tympanic membrane opacification and loss of the light reflex. Moreover, the tympanic membrane may retract and become less mobile. Tympanoplasty with modified cartilage augmentation may be necessary if substantial tympanic membrane retraction is seen in order to stop the development of a retraction pocket.
Evaluation of Chronic Otitis Media Effusion
Tympanometry and audiometry tests should be performed on patients with otitis media with effusion according to their age. An otitis media with effusion diagnosis will be supported by a “flat” tympanogram. [Auditory brainstem responses can be used to examine a baby’s hearing (ABR). This examination measures the brainstem’s electrical response to sounds. The test measures both the frequency range and the degrees of sound intensity at which the patient’s brain reacts. For the test to be completed, patients do not even need to be awake or able to communicate. It is therefore perfect for kids from infancy to five years old.
Although ABR testing can still be done on older children and adults with Chronic Otitis Media Effusion a conventional audiology test is more frequently conducted in these cases. During this examination, sounds in various tones and intensities are played to the patient’s left and right ears. When a sound is heard in the right or left ear, the patient is instructed to raise their hand in that direction. The patient’s typical hearing levels and frequency range will be determined by the results.
A normal person needs a sound to be louder to notice high frequencies than low frequencies because those with normal hearing can detect lower frequencies at a lower decibel (i.e., strength) than higher frequencies. An audiograph is used to plot the range of frequencies that a person can hear during an audiology examination. Individuals with OME have a lower decibel (dB) range in the audiograph.
Levels of hearing loss (a decline in hearing thresholds from baseline levels) for Chronic Otitis Media Effusion
26–40 dB for slight impairment.
41–60 dB for moderate impairment
61–80 dB for severe disability.
71-90 dB for severe hearing loss
Deafness and severe impairment: 81 dB or greater. [12]
Management / Treatment of Chronic Otitis Media Effusion-
Otitis media with effusion typically goes away on its own with careful observation. Myringotomy with tympanostomy tube insertion is thought to be an effective treatment if it is persistent, though. A ventilation tube is used in this procedure to get air into the middle ear, which prevents fluid from building up again. Due to the growth and development of the Eustachian tube angle, which will enable drainage, many patients won’t require further therapy after this procedure.
DISCLAIMER-Some patients go to net and directly take treatment from there which can lead to catastrophic consequences-Then- Many people ask then why to read all this text -the reason is that it helps you to understand the pathology better ,you can cooperate with treatment better ,your treating physician is already busy with his patients and he does not have sufficient time to explain you all the things right from ABCD ,so it is always better to have some knowledge of the disease /disorder you are suffering from.
Adenoidectomy is currently used to treat patients of Chronic Otitis Media Effusion- who have enlarged adenoids, and it is a crucial addition to their care.
Language development may be impacted by hearing loss in children. As a result, using hearing aids as a non-invasive treatment for OME may be considered.
A number of factors are taken into consideration by clinicians when deciding which Chronic Otitis Media Effusion interventional treatment is best for a given patient.
Conditions that the patient has
How severe your hearing loss is
unilateral or bilateral OME presence
Duration of effusion
Patient’s age Social variables
Patient expense
Probability of patient adherence to treatment
family support for the therapy
Assessing hearing impairment should be done with a patient-centered mindset. The child’s social and academic adjustment is more crucial than the findings of audiometry tests. Both physical and social aspects should be considered in order to give a patient-centered treatment plan that maximises outcomes for the patient, even if the majority of OME patients will warrant a conservative management approach as opposed to more intrusive procedures.

Multiple Diagnoses for Chronic Otitis Media Effusion
It is important to distinguish OME from acute otitis media, and in adults, OME can be brought on by a nasopharyngeal cancer that has invaded the Eustachian tube.
Operative Oncology
Although patients with may show no signs or symptoms other for the loss of hearing associated with ,Chronic Otitis Media Effusion 5.7% of patients develop the OME due to an obstruction caused by a nasopharyngeal cancer. It is advised that OME patients have their nasopharynx and external acoustic meatus examined. A postnasal space biopsy is advised if abnormalities in the nasopharynx are seen.
Oncology of Radiation
Radiation therapy can cause Chronic Otitis Media Effusion in nasopharyngeal cancer patients. This particular OME could last for several months. To further understand the chances of getting OME after radiation therapy and how irradiation dosages might affect this consequence, more research is required.
Relevant Research and Active Trials
Finding OME treatment options that work has involved experimenting with a variety of therapies. Oral steroids for children have showed some promise. It is unclear, nevertheless, whether these advantages are clinically meaningful. Otic drops have also been used to preserve the patency of tympanostomy tubes. In these studies, the occlusion rate between patients receiving pharmacological therapy and those in the control (no drug) circumstances did not differ statistically.
Arrangement of Care
OME is not typically caused by bacterial infections but rather by viral or allergy-related causes. Antibiotic usage is not advised as a result. Moreover, it has not been demonstrated that using corticoids to treat allergies has a substantial effect on how OME affects patients. Antibiotics and corticoids are not advised for the treatment of Chronic Otitis Media Effusion due to these factors. Watchful waiting for three months is the best course of action for OME sufferers. A specialist referral may be made to evaluate surgical treatment options in cases when OME continues.
Treatment of Toxicities and Adverse Effects regarding Chronic Otitis Media Effusion
If ototopical drops get inside the inner ear and into the middle ear, they may cause ototoxicity. Ototopical drops are not typically used to treat OME, though.
Health Oncology
Radiation following nasopharyngeal cancer might generate numerous problems. The most typical side effect is xerostomia (i.e., dry mouth caused by a lack of saliva). In some situations, a persistent OME might emerge, necessitating additional treatment or surgical intervention.
Prognosis
OME cases typically end on their own. In severe situations, the illness impairs the patient’s hearing. As a result, sociability and communication may suffer. Deficits in hearing in early children may result in delayed language development or learning issues. The impact of OME on these factors has not been completely researched. Chronic Otitis Media Effusion might cause unusual side effects include clumsiness, behavioural issues, and dizziness.
Complications
With continued OME, long-term alterations to the middle ear and tympanic membrane may take place, leading to permanent hearing loss. The use of ventilation tubes aims to reduce these long-term consequences. Yet, issues like tympanosclerosis might develop even in patients who have had treatment.
Care following surgery and rehabilitation
Eustachian tube rehabilitation may be helpful in managing Chronic Otitis Media Effusion in addition to medication and surgical therapy. Exercises for breathing, education about improving nasal cleanliness, and auto-insufflation for the tensor veli palatini and levator veli palatini muscles can all be used to treat the Eustachian tube.
Consultations for Chronic Otitis Media Effusion
To ensure that these patients receive comprehensive care, OME must maintain relationships with a wide range of medical specialists, such as audiologists and otolaryngologists. Many medical professionals and parents favour non-invasive treatments, such as the use of hearing aids, to prevent the possibility of breathing tube issues. When a patient’s audiometry indicates normal hearing and they don’t have any speech, language, or developmental issues, reassuring them and explaining the “watchful waiting” strategy is a crucial element of management. If “watchful waiting” is used, the patient should be closely monitored for changes in symptoms or indications of increased pressure on the tympanic membrane because rupture would have a negative impact on the patient’s chances of passing a future audition.
The middle ear’s anatomy should be explained to and understood by parents of children with recurrent OME. When engaging in these activities, the head position can be adjusted to promote adequate drainage and help the kid avoid further bouts of OME.
Improving Healthcare Team Results for Chronic Otitis Media Effusion
OME treatment objectives include reducing middle ear fluid, enhancing hearing, and averting further episodes. The identification of the best treatment regimens for patients with OME will always be aided by physicians’ dialogue with patients, nurse practitioners, patients, and patients’ families.
Children in whom “watchful waiting” is the chosen method should undergo reevaluation every three to six months until the effusion resolves or intervention is necessary. Also, families should be made aware of the symptoms and indicators of a pathology that has advanced. In these situations, further discussions regarding modifications to the treatment plan may be necessary. The majority of kids have positive outcomes.
Persistent Otitis Media in Adults
The middle ear may experience chronic otitis media, which is a persistent infection or inflammation, in both adults and children.
Young, developing children are frequently afflicted by chronic suppurative otitis media, also known as chronic otitis media or a chronic middle ear infection. But this illness can also affect adults. A middle ear infection that persists or recurs frequently is referred to as chronic otitis media, and if left untreated, it can lead to hearing loss and other severe consequences.
Causes of persistent otitis media
An acute middle ear infection frequently progresses to chronic otitis media. Chronic otitis media may be caused by a blocked Eustachian tube—the channel that connects the rear of the nose to the middle ear—or an injury to the ear.
Chronic otitis media can affect anyone over the age of 18, but the risk is higher for those who:
- Smoke or are often in the company of smokers
- Experience allergies all year long or only during certain seasons
- Are frequently exposed to air pollution
Symptoms of Persistent Otitis Media
Chronic otitis media symptoms usually manifest as “flare-ups” that may occur after an upper respiratory infection, another ear infection, or an excessive amount of water entering the ear.
In contrast to the well-known agony of acute middle ear infections, chronic otitis media is often painless (although some individuals do have discomfort in one or both ears).
The most typical signs and symptoms are:
- Discharge from the ear that resembles pus
- A painful throat
- Bad, muffled hearing
- Difficulty falling asleep
- Temperature
Leaving an acute middle ear infection or chronic otitis media untreated can lead to substantial damage to the ear’s hearing bones (ossicles) and hearing loss, so it’s crucial to seek medical care right away if you experience any symptoms.
Diagnosis of Chronic Otitis Media
A comprehensive review of symptoms and medical history, as well as an ear examination, are the first steps in determining whether a middle ear infection is chronic. A diagnosis of chronic otitis media may be made if pus is building up close to the eardrum or other signs are present.
Treatment for Chronic Otitis Media
Antibiotics are the primary course of treatment for chronic otitis media. Although some patients may receive a course of oral antibiotics, antibiotic ear drops are usually prescribed. Surgery may be advised in more severe cases to:
- Fix a fractured eardrum and/or hearing bones
- Take away infected tissue.
- Introduce a little tube into the ear to enhance airflow and drainage
Patients with chronic otitis media and other complicated ENT diseases receive comprehensive care from the otolaryngologists, surgeons, nurses, and other specialists at the ENT & Urology Institute at Tampa General Hospital.
Chronic Suppurative Otitis Media
- The assessment of a physician
If pus or skin-like stuff gathers in a hole or pocket in the eardrum and the material tends to drain, a doctor will diagnose chronic suppurative otitis media. Doctors collect samples of the discharge from the ear to determine which bacteria are responsible for the illness.
If a patient is suspected of having a cholesteatoma, a computed tomography (CT) scan or a magnetic resonance imaging (MRI) scan may be performed. Physicians may perform a biopsy to look for tumors in patients with persistent or recurrent granulation tissue (new tissue that develops on the healing surface of the eardrum).
Management of persistent suppurative otitis media
- Ear drops with antibiotics
- Occasionally, antibiotics are taken orally.
Antibiotic ear drops are administered by physicians when chronic suppurative otitis media flares up. Antibiotics are also administered orally to those who experience severe flare-ups. When there is a hole, the ear needs to be kept dry, save for prescribed ear drops. To prevent water from entering the ear while taking a bath or shower, people are advised to insert a cotton ball covered in petroleum jelly into their ear. Avoid going swimming.
A surgical operation called tympanoplasty is often used to fix the eardrum perforation. In the event that the ossicles have been damaged, they can be fixed at the same moment.
The middle ear structures must be rebuilt, and a cholesteatoma must be surgically removed. Severe problems can arise in other ways, including polyps, damage to the ossicles or other bones, and the spread of infection. A second surgery is performed to determine if the cholesteatoma has returned before beginning reconstruction because it can recur.
If any patient has any ENT -Ear nose throat problems and requires any , consultation ,online consultation ,or surgery in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may TAKE APPOINTMENT BY CLICKING ON THE LINK GIVEN BELOW-
Clinic address of ENT SPECIALIST doctor Dr Sagar Rajkuwar-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road ,Ambad ,1 km from Pathardi phata Nashik ,422010 ,Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cel no- 7387590194 , 9892596635


