
Middle Ear Tumor-various aspects-
Middle ear tumors, which are usually benign, may include glomus tumors (paragangliomas) and schwannomas, but they can also encompass cholesteatomas and, infrequently, adenomas or squamous cell carcinomas.
Here’s a more detailed explanation:
Types of Middle Ear Tumors:
Glomus Tumors (Paragangliomas):
These represent the most prevalent primary tumors of the middle ear.
They are generally benign and grow slowly.
They arise from paraganglia, which are clusters of nerve tissue that react to variations in body temperature or blood pressure.
They are frequently located in the vicinity of the cochlea and vestibular system.
Symptoms: Hearing issues or loss, ringing or pulsating sounds in the ear (pulsatile tinnitus).
Schwannomas:
These tumors form from the schwann cells, which are nerve cells that create the myelin sheath that covers nerve fibers.
They can arise anywhere along the path of the facial nerve.
Cholesteatomas:
These are benign yet potentially harmful growths of skin cells that can develop in the middle ear.
They may damage ear structures and can lead to hearing loss, ear drainage, and additional complications.
Adenomas:
These are uncommon, noncancerous tumors that arise in the middle ear.
They originate from middle ear mucosal cells that have both epithelial and neuroendocrine characteristics.
Squamous Cell Carcinoma:
This is an unusual type of cancer that may occur in the middle ear.
It is the most frequent variety of ear cancer.
Symptoms of Middle Ear Tumors:
Hearing loss
Ringing or pulsating sounds in the ear (pulsatile tinnitus)
Dizziness
Facial nerve weakness
Pain
Ear drainage
Diagnosis and Treatment:
Diagnosis: Physical examination, imaging scans (including CT and MRI), and potentially a biopsy.
Treatment:
Glomus Tumors: Surgical excision, Gamma Knife radiosurgery, or a combination of both.
Other Tumors: Treatment varies based on the tumor type and stage and may involve surgery, radiation therapy, or chemotherapy.
Important Notes:
The majority of ear tumors are benign (non-cancerous).
Early detection and management are crucial to avoid complications.
If you notice any symptoms of a middle ear tumor, seek advice from a healthcare provider.
If Any Patient of ENT Requires Any Surgery, Opd Consultation Or Online Consultation In Clinic of ENT Specialist Doctor Dr. Sagar Rajkuwar ,He May Contact Him At The Following Address-
Prabha ENT Clinic, Plot no 345,Saigram Colony, Opposite Indoline Furniture Ambad Link Road ,Ambad ,1 km From Pathardi Phata Nashik ,422010 ,Maharashtra, India-Dr. Sagar Rajkuwar (MS-ENT), Cell No- 7387590194, 9892596635
Ear Tumors
Tumors in the ear can develop on your outer ear (skin cancer), inner ear, or middle ear. The majority of ear tumors are benign (non-cancerous), but they might lead to hearing loss. Although small benign tumors typically don’t need treatment unless they produce symptoms, all cancerous tumors do require intervention. Treatment options include Mohs surgery, radiosurgery, and radiation therapy.
Overview
What is an ear tumor?
An ear tumor is a growth or lump of atypical cells that develops in your ear. The majority of ear tumors are benign, meaning they are not cancerous. However, some ear tumors are malignant (cancerous).
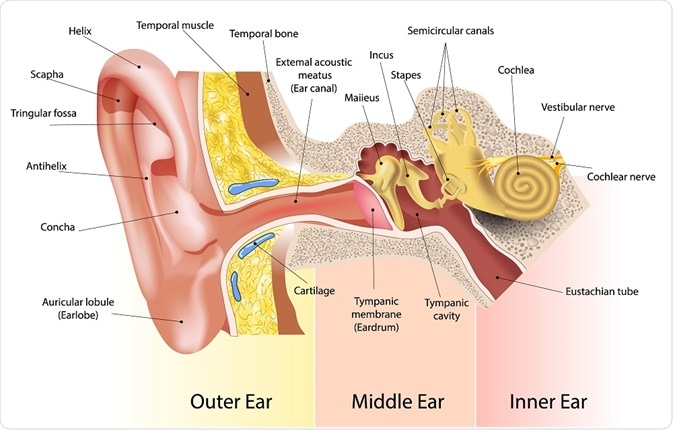
Ear tumors can occur in any area of your ear, including the inner ear, middle ear, or outer ear. They may impact your hearing. It is crucial to have tumors evaluated promptly, before they potentially lead to long-lasting problems.
What’s the difference between an ear cyst and an ear tumor?
Both cysts and tumors can lead to a bump or lump on or within your ear:
Cysts are small sacs that typically contain fluid and are generally not cancerous. The most common ear cysts are sebaceous cysts (epidermal inclusion cysts). They can appear in your ear canal, behind your ear, or on your earlobe.
Tumors are solid tissue masses that may be cancerous or noncancerous. Most ear tumors are benign growths that occur on your outer ear.
Types of benign (noncancerous) ear tumors
Noncancerous ear tumors can obstruct your ear canal, resulting in earwax accumulation. Certain types that arise within your ear can grow sufficiently large to damage the organs responsible for hearing and balancing:
Acoustic neuromas (also known as vestibular schwannomas) develop on your vestibulocochlear nerve. This nerve in your inner ear connects to your brain.
Adenomas are uncommon noncancerous tumors that form in your middle ear.
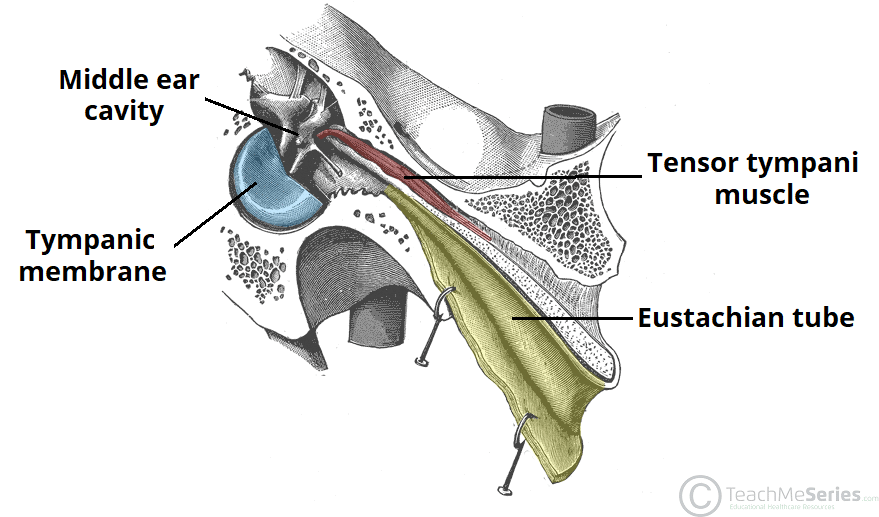
Cholesteatomas are sacs filled with fluid, air, or skin cells that occur behind your eardrum in your middle ear. They can lead to hearing impairment if untreated.
Exostoses and osteomas are benign bone tumors that arise on the bones in your external ear canal.
Glomus tympanicum paraganglioma affects your tympanic nerve. This nerve in your middle ear connects to your eardrum.
Keloids are a type of fibrous scar tissue. They can develop after an ear piercing or injury to your outer ear.
Types of malignant (cancerous) ear tumors
Cancer can develop inside or on the external part of your ear. However, ear cancer is uncommon.
The majority of cancer that affects your ear is, in fact, skin cancer. Around 6% to 10% of skin cancers originate on the outer ear. Skin cancers that may involve your ear include:
Basal cell carcinoma.
Melanoma.
Squamous cell carcinoma.
Cancers that directly impact your middle or inner ear are even rarer:
Adenoid cystic carcinoma is a rare cancer that typically forms in your salivary glands. In even rarer occurrences, it may develop in your ear canal.
Ceruminous adenoma arises in the cells responsible for producing earwax. This cancer does not spread, but it can damage sections of your ear canal.
Rhabdomyosarcoma is an uncommon pediatric cancer that affects muscle tissue. It may manifest in your head or neck, including your middle ear.
Symptoms and Causes
What are the symptoms of an ear tumor?
Symptoms of an ear tumor differ based on the tumor type and the specific part of your ear it influences. Indications of an ear tumor include:
A lump on the outer section of your ear.
Vertigo or issues with balance.
Bleeding or discharge from the ear.
Pain in the ear.
Migraines.
Loss of hearing.
Wound or sore that does not heal.
Changes in skin color, newly formed moles, or alterations to an existing mole.
Lymph nodes that are swollen.
Tinnitus (a ringing sound in your ears).
Weakened muscles in the face.
For update on further important health related topics and frequently asked questions on health topics by general population please click on the link given below to join our WhatsApp group –
https://chat.whatsapp.com/Lv3NbcguOBS5ow6X9DpMMA
What leads to the formation of an ear tumor?
Ear tumors arise when your body produces new cells at an accelerated rate. Occasionally, older, damaged cells fail to die as they should. Bunches of both old and new cells cluster together, creating a tumor.
Cancerous ear tumors develop when the cells proliferate uncontrollably. Without treatment, these malignant cells might spread to other areas of your body (metastatic cancer).
Risk factors for ear tumors
Individuals across all age groups, including children, can develop ear tumors. Factors that heighten your risk of forming an ear tumor comprise:

Chronic ear infections.
Ear piercings.
Genetic conditions, like neurofibromatosis (NFS).
Previous exposure to radiation.
Repeatedly being in cold water, such as from scuba diving (surfer’s ear).
Tobacco use, including secondhand smoke exposure.
What complications can arise from ear tumors?
Ear tumors, including those that are not cancerous, may result in hearing loss. They can lead to frequent infections and affect the inner ear structures responsible for hearing and balance.
Your healthcare provider can guide you on when it is appropriate to monitor a tumor and when treatment is necessary to avoid complications such as these.
Diagnosis and Tests
How are ear tumors identified?
Your healthcare provider may detect a tumor by checking your ear during a physical assessment. They might refer you to an audiologist (a hearing specialist) for a hearing examination. You will probably also consult an ear, nose, and throat doctor (an ENT or otolaryngologist) who focuses on ear ailments.
If your provider thinks your ear tumor could be malignant, they will conduct a biopsy. This process extracts the tumor or cells from the tumor. A pathologist (a physician who analyzes diseases) reviews the samples in a laboratory to arrive at a diagnosis.
Since inner ear tumors are challenging to access and biopsy, your provider may request a CT scan or MRI for further information about them. In rare instances, surgery may be necessary to remove the tumor before a provider can diagnose it.
Management and Treatment
How are benign ear tumors managed?
Some noncancerous ear tumors don’t require intervention unless the tumor impacts your hearing or balance. Your healthcare provider may observe the tumor to monitor its growth and inquire about any symptoms you’re facing.
The most frequent treatments involve removing the growth via surgery or other techniques. For instance, providers commonly use radiosurgery (gamma knife surgery) to eliminate benign ear tumors such as acoustic neuromas. This method targets high doses of radiation directly onto the tumor. It isn’t surgery, yet it eradicates tumors with precision akin to surgical methods.
To address keloids, your healthcare provider might inject the tumor with a corticosteroid. Some keloids may necessitate surgical excision followed by radiation therapy to eliminate any remaining cells.
How are malignant ear tumors treated?
Dermatologists (physicians specialized in skin diseases) treat skin cancer affecting the outer ear. Treatment options for cancerous ear tumors depend on the type and location of the cancer. Possible treatments include:
Mohs surgery to eliminate the cancerous skin cells.
Radiation therapy, radiosurgery, or chemotherapy to eradicate cancer cells.
Surgery to excise tumors and (possibly) adjacent lymph nodes where cancer cells could have disseminated.
Prognosis
What’s the outlook for individuals with ear tumors?
Small ear tumors that aren’t producing symptoms may not require treatment at all. However, if a tumor is leading to hearing loss or other complications, surgical removal might be necessary. Most individuals who undergo surgery or alternative treatments for benign ear tumors recover satisfactorily.
The prognosis for ear cancer hinges on factors like the type of tumor, its location, and its stage (the extent of its spread). Nonetheless, even with melanoma (the most lethal type of skin cancer), the five-year survival rate is 99% when surgery successfully removes the cancer before it has metastasized.
Skin cancer on the outer ear can occasionally recur and spread to other areas of your body. Regular skin examinations will be essential to monitor for any returning cancer.
Living With
When should I consult my healthcare provider?
Contact your healthcare provider if you experience:
Balance issues or dizziness.
Ear bleeding, discharge, or discomfort.
Hearing impairment.
Ringing in the ears (tinnitus).
Changes in the skin of your ear, including a new lump, mole, or sore.
What questions should I pose to my healthcare provider?
You may wish to inquire with your healthcare provider:
Is my ear tumor malignant or benign?
What type of ear tumor do I have?
What’s the most suitable treatment for me?
What are the risks and side effects associated with the treatment?
Should I be alert for signs of complications?
What is the most common tumor in the middle ear?
The paraganglioma, often called the glomus tumor, is the most prevalent tumor of the middle ear and the second most frequent tumor located in the temporal bone. Chemodectoma is an alternative term that is sometimes utilized to refer to this tumor.
What are the symptoms of a tumor in the ear?
When ought I to consult my healthcare provider?
Issues with balance or feelings of dizziness.
Bleeding from the ear, discharge, or discomfort.
Loss of hearing.
A ringing sensation in the ears (tinnitus).
Alterations in the skin of your ear, such as a new lump, mole, or sore.
Radiation treatment
The treatment of an acoustic neuroma involves the use of a variety of radiation therapy methods:
- Stereotactic radiosurgery. An acoustic neuroma may be treated using stereotactic radiosurgery, a kind of radiation therapy. It is frequently employed when the tumor is tiny, measuring less than 2.5 cm in diameter. If you are an older adult or unable to undergo surgery due to health concerns, radiation therapy may be an option.
Using several tiny gamma rays, stereotactic radiosurgery, which includes Cyber Knife and Gamma Knife, provides a precisely targeted dose of radiation to a tumor. With this approach, therapy is provided without causing tissue damage or requiring an incision.
The aim of stereotactic radiosurgery is to halt the development of a tumor, protect the function of the facial nerve, and maybe save hearing.
The consequences of radiosurgery might not be apparent for weeks, months, or even years. Your health care team keeps track of your progress by performing hearing tests and follow-up imaging examinations.
Radio surgery has several dangers, such as:
- Hearing loss.
- ear ringing.
- numbness or weakness in the face.
- Issues with balance.
- Tumor growth that persists.
Stereotactic radiotherapy by fractionation. Over many treatments, fractionated stereotactic radiotherapy (SRT) delivers a modest radiation dose to the tumor. The goal of SRT is to halt tumor growth without harming surrounding brain tissue.
proton beam treatment. This radiation therapy approach employs high-energy beams of positively charged particles known as protons. To treat tumors, the afflicted region receives precisely targeted doses of proton radiation. This method of treatment reduces radiation exposure to the surrounding environment.
Therapy that provides support
Supportive therapies can aid in addition to treatment aimed at eliminating or halting the tumor’s growth. Supportive therapies treat the signs and symptoms of an acoustic neuroma and its treatment, such as vertigo or balance issues.
Hearing loss can be treated with cochlear implants or other methods.
Key Arguments
- Middle ear adenomatous tumors can cause a wide range of symptoms, the most typical of which is conductive hearing loss.
- Adenomatous middle ear tumors are difficult to diagnose clinically due to potential overlap with other illnesses, such as paraganglioma.
- Although magnetic resonance imaging and computed tomography may be helpful, no imaging procedure can definitively diagnose adenomatous middle ear tumors.
- Whether middle ear adenomatous tumors should be classified is up for discussion, and there is a lot of disagreement on the subject.
Pathogenesis
It’s unknown what the precursor cell is for adenomatous middle ear tumors. Derlacki and Barney proposed that middle ear adenoma originated from the surface epithelium mucosa, as did Hyams and Michaels. Middle ear adenomas have also been proposed to arise from displaced or trapped embryonic rests of glandular cells in the middle ear mucosa, and some researchers have hypothesized that these embryonic cells originate from the neural crest.
The connection between the middle ear and other reports has been deemphasized.
Immunohistochemistry and microscopy
Middle ear adenomas and carcinoid tumors have been described using light microscopy with similar, sometimes indistinguishable, morphologies. Despite the fact that prevalent architectural patterns may differ from one tumor to another and inside the same tumor, they are typically organized into trabeculae, glandular spaces, festoons, ribbonlike patterns, anastomosing cords, and solid sheets. The cells of both tumors are characterized as cuboidal to columnar, homogeneous in size, and with eosinophilic, finely granular cytoplasm.
Classification
There is no widely accepted classification system for adenomatous middle ear tumors in the literature. Saliba and Evrard11 presented one recently suggested approach, in which middle ear glandular tumors were categorized into three subtypes. The neuroendocrine adenoma of the middle ear is the most prevalent neoplasm (type I). It has negative metastasis but positive immunohistochemistry. The middle ear adenoma, which exhibits negative immunohistochemistry and no metastasis, is a kind of type II tumor.
Middle Ear
The majority of otologic specimens sent to the surgical pathology lab are inflammatory products. Due to the possibility that congenital, inflammatory, reactive, and neoplastic lesions in the middle ear can all manifest with similar symptoms (fullness, tinnitus, pain, hearing loss, discharge), imaging signs of a mass lesion with or without bone erosion, and, pathologically, as an inflamed or necrotic mass, the pathologist may be perplexed by these inflammatory tissues from the middle ear or mastoid. In order to avoid missing a necrotic tumor, a differential diagnosis of the biopsy material necessitates a thorough understanding of the clinical and imaging data. This is especially true for youngsters, who are very uncommon tumors and are frequently misdiagnosed as inflammation at first.
Fundamental knowledge about the origin and transmission of middle and inner ear illness has come from pathologic studies of temporal bones collected during autopsy. The temporal bone may be clinically dissected using modern imaging procedures, and neurotologic methods can be used to biopsy localized illness.
Click on the link below to learn more about this disease.
FOR FURTHER INFORMATION IN GREAT DETAIL ON Middle ear implants PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
FOR FURTHER INFORMATION IN GREAT DETAIL ON Can we put coconut oil in ear PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
If Any Patient of ENT Requires Any Surgery, Opd Consultation Or Online Consultation In Clinic of ENT Specialist Doctor Dr. Sagar Rajkuwar ,He May Contact Him At The Following Address-
Prabha ENT Clinic, Plot no 345,Saigram Colony, Opposite Indoline Furniture Ambad Link Road ,Ambad ,1 km From Pathardi Phata Nashik ,422010 ,Maharashtra, India-Dr. Sagar Rajkuwar (MS-ENT), Cell No- 7387590194, 9892596635
Issued in public interest by –
www.entspecialistinnashik.com


