
Mastoid obliteration surgery-various aspects-
Mastoid obliteration
What is mastoid obliteration?
You have been advised to undergo mastoid cavity obliteration surgery to remove a problematic mastoid cavity. The primary cause of a problematic mastoid cavity is repeated or ongoing infections.
In this document, we outline some of the objectives, advantages, risks, and alternatives associated with the suggested procedure. The procedure itself will also be detailed.
We aim for you to be aware of your options so that you can be completely engaged in making any decisions regarding your procedure. Please inquire about anything you do not completely understand or would like to have clarified further.
For update on further important health related topics and frequently asked questions on health topics by general population please click on the link given below to join our WhatsApp group –
https://chat.whatsapp.com/Lv3NbcguOBS5ow6X9DpMMA
Issued in public interest by –
How does the ear work?
The ear is made up of the outer, middle, and inner ear. Sound moves through the outer ear and arrives at the eardrum, making it vibrate. This vibration is then passed on through three small bones known as the ossicles, located in the middle ear.

The vibration subsequently enters the inner ear, which is a spiral-shaped bony structure filled with fluid. The nerve cells inside the inner ear are activated to create signals that are sent to the brain, where they are understood as sound.
What is the mastoid bone?
The mastoid bone is the bony protrusion that is palpable just behind the ear (see diagram).
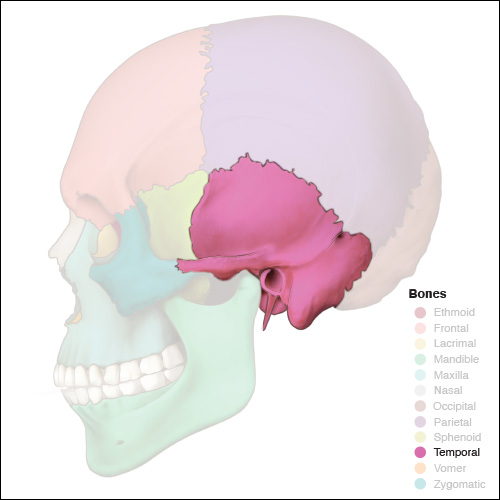
Image of mastoid bone
It encompasses several air cavities, the biggest of which is referred to as the antrum, and links with the air space in the middle ear.
Ear infections in the middle ear may spread into the mastoid bone.
Why have I been referred for mastoid cavity obliteration?
Following your earlier procedure, one or more components in your ear (such as the ear drum, ossicles, and a portion of your mastoid bone) have been excised, leading to the formation of a mastoid cavity.
Mastoid obliteration surgery has been advised for you since your mastoid cavity is persistently discharging or gathering dead skin, and it has not improved despite routine cleaning and antibiotic drops.
The aim of this surgery is to eliminate the disease from your ear, whether it involves infected tissue or cholesteatoma (dead skin that accumulates in your ear and can damage the surrounding structures), and subsequently to reconstruct your ear.

What are the intended benefits of mastoid cavity obliteration?
• The primary advantage of this procedure is to provide you with a dry, waterproof, and hassle-free ear.
• Occasionally, if the hearing function of your inner ear remains operational, it might be feasible to enhance your hearing in the impacted ear. Your surgeon will be capable of advising and conversing about this with you. It is not always feasible to enhance hearing, even when the hearing capability of your inner ear continues to function.
How successful is this procedure?
About 85 out of every 100 patients will experience a dry, problem-free ear following this surgery. We also aim to enhance your hearing. The likelihood of enhancing your hearing is around 60 out of 100 patients. If your hearing cannot be enhanced, a secure, dry waterproof ear may permit you to use a hearing aid or your surgeon might suggest another hearing option after recovery.
Who will perform my procedure?
An otolaryngologist (ENT) surgeon, possessing the necessary experience, will carry out your procedure.
What will happen before my procedure?
• Most patients visit a pre-admission clinic run by a nurse, a few days or weeks prior to their surgery.
• During this clinic, we will request information regarding your medical history and perform any required clinical examinations and tests such as measuring your blood pressure, pulse, and weight. This is a great chance for you to inquire about your procedure, but don’t hesitate to share any concerns at any time.
• You will be inquired if you are taking any pills or other medication, which could be ones prescribed by a physician or purchased over the counter at a pharmacy. It is beneficial if you bring information about any medications or supplements you are currently taking.
• Quitting smoking aids in faster healing after your surgery, among other advantages. The Stop Smoking Service provides free support, so please request a referral if you are interested.
Will I have an anaesthetic?
Yes. This process requires a general anaesthetic, indicating that you will be unconscious during your procedure.
Will I have to stay in hospital overnight?
Most individuals undergoing this kind of procedure are able to return home on the same day as their operation. Occasionally, we are aware prior to your surgery if you will require a longer stay than normal; your physician will talk about this with you before you make the decision to proceed with the surgery.
Does some of my hair need to be removed before my procedure?
The healthcare team must access the skin located behind your ear for the procedure. Therefore, they will likely have to employ an electric hair clipper (equipped with a single-use disposable head) to cut some of your hair on the day of the surgery. Kindly refrain from shaving the hair on your own as this may elevate the risk of skin infection.
You will be instructed to shower and cleanse your hair either the evening prior to or on the morning of your procedure.
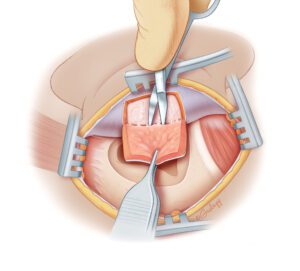
What happens during the operation?
The surgery is conducted under general anesthesia and may last up to five hours.
After you become unconscious, an incision (cut) is made behind your ear, and the infected tissues in the mastoid, along with cholesteatoma (dead skin), are excised to expose healthy bone. If the surgeon identifies any leftover (residual) infection, the infected bone will be removed through drilling.
At this stage, synthetic bone substitute, or your own bone dust or chips, is utilized to fill the cavity. The filling material is subsequently covered with cartilage and local soft tissue flaps to assist in creating a healthy ear canal.
Your surgeon may often restore your eardrum using cartilage, depending on which structures remain available and healthy in your ear. If there is potential for improving your hearing, the ossicular chain (bones of hearing) may be substituted with a prosthetic (artificial) ossicle made of titanium. These prostheses are compatible with MRI scans. This will be discussed with you during your clinic appointments; however, it is frequently impossible to determine if this option is viable until the actual operation.
The ear is then packed with ribbon gauze, saturated with antiseptic paste, to secure the graft in position. The wound is sutured with dissolvable stitches, and an adhesive dressing (steristrips) is placed to safeguard it. A cushioned bandage is applied and left on overnight. Your surgeon will typically recommend that you remove this at home.
Are there alternatives to this procedure?
The sole method to ensure that you will not encounter additional issues stemming from your mastoid cavity is through the removal of the cavity (obliteration). For patients who are not suitable for this procedure, the only option is to have a specialist consistently clean the ear and for the patient to apply antibiotic ear drops or creams. This, at most, might lessen the discharge.
Are there any significant, unavoidable, or frequently occurring risks of mastoid cavity obliteration surgery?
There are certain risks that you need to think about before consenting to this treatment. You ought to converse with your surgeon regarding the likelihood of any complications in your situation.
• Scar
You will have a scar located behind your ear. Initially, this will appear red or pink but will gradually fade to a white hue over time, making it less noticeable. This scar might cause discomfort for some duration following your surgery, frequently lasting several months. You might feel some numbness in the area around the scar, which may or may not improve over time. Occasionally, a scar can become larger than it was right after the surgery (hypertrophic or keloid), which could require an additional procedure at a future date.
• Bleeding
You might notice some bloodstained discharge from your ear during the weeks after your surgery. If the bleeding does not stop, please reach out to Rotary Ward using the number provided at the end of this leaflet and request to speak to the on-call ENT doctor.
• Loss of hearing
In a small percentage of patients, hearing may deteriorate due to injury to the inner ear. It is possible that you may experience complete and permanent loss of hearing in the ear that is being operated on (which is sometimes referred to as a dead ear).
• Dizziness
Dizziness is frequently experienced for several hours after surgery to obliterate the mastoid cavity and may lead to nausea (a feeling of sickness) and vomiting. In rare cases, dizziness can be severe and ongoing, requiring a longer hospitalization and specialized physiotherapy.
• Tinnitus
Sometimes a patient may detect sounds in their ear, especially if their hearing loss worsens. This sound is referred to as tinnitus and can be either temporary or permanent.
• Weakness of one side of the face
The nerve responsible for controlling the movement of facial muscles runs within the ear and may sustain damage during your surgery. If this occurs, the movement on the side of the operation may be affected, but it is typically temporary. A facial nerve monitor is utilized during your procedure to help minimize the risk of nerve injury. There is a very low risk of permanent paralysis on one side of the face.
• Taste disturbance
The nerve responsible for taste is located near the eardrum and may occasionally sustain damage. This can result in an unusual taste on one side of your tongue. This condition is usually temporary, although it can be permanent in approximately one in ten affected patients.
• Cerebrospinal fluid leak
The brain is situated above the mastoid bone, encased in a fluid known as cerebrospinal fluid or CSF. On rare occasions, ear disease might erode the bone separating the mastoid from the brain, or the bone can be compromised during surgery. If a CSF leak is identified during the operation, it is repaired at that time. Sometimes the leak may manifest later, necessitating an additional surgical procedure.
• Reaction to ear dressings
Occasionally, your ear may experience an allergic reaction to the dressings applied in your ear canal. If this occurs, the pinna (outer ear) may swell, become red, and itch. In such cases, you should consult with your surgeon so that they can remove the dressing from your ear. The allergic reaction typically resolves after a few days.
• Change in shape of the ear
The cartilage utilized to obliterate the cavity will be harvested from your ear during surgery. This is performed in a manner that is not noticeable in most instances. However, there is a slight risk that the shape of your ear may change marginally due to the removal of some of this cartilage.
• Haematoma formation
A haematoma is a collection of blood beneath the skin. If this occurs on or around your ear, it may require removal through a small additional procedure to prevent deformity of your ear or the development of an infection.
There are universal risks associated with all major surgeries due to the administration of general anesthesia. These can be discussed with your anesthetist prior to your surgery.
The development of blood clots in your legs or lungs are also general risks associated with undergoing surgery. As part of your pre-admission evaluations, you will be assessed for the risk of developing clots in your legs (deep vein thrombosis or DVT) or lungs (pulmonary embolism or PE), and options for reducing these risks will be provided.
will be talked about with you.
You can reconsider your decision regarding the operation at any point, and signing a consent form does not obligate you to proceed with the operation.
If you desire to obtain a second opinion concerning your treatment, you can request this from your specialist; they will be happy to facilitate this for you. You might also want to ask your own GP to help arrange a second opinion with a different specialist.
Will I be in pain after my procedure?
Your surgeon will administer an injection around your ear prior to the start of your operation, which will minimize your pain following the surgery. You might experience some discomfort in your ear after your procedure, but this can be managed with painkillers that we will request you to purchase, like paracetamol and ibuprofen. Additional painkillers may be given by the hospital before you leave.
When can I resume normal activities?
We will assist you in getting mobile as quickly as possible following your procedure. This aids in enhancing your recovery and lowers the likelihood of specific complications.
When can I return to work?
You might have to take two to four weeks away from work or school following your surgery.
When can I leave hospital?
You will typically return home on the same day. You will have a head dressing that you can take off the following day, but you need to keep the packing in your ear. You should consult your surgeon if you suddenly notice deafness, dizziness, or intense pain after being discharged from the hospital.
How do I look after my wound following my procedure?
• Generally, there are no stitches to take out. The stitches utilized are located beneath your skin and will dissolve naturally over time.
• You might have some adhesive strips over your wound that you can take off approximately seven days post-operation. If they come off before this timeframe, there’s no cause for concern, and they do not require replacing.
• There could be a minor amount of discharge from your ear canal. This typically originates from the dressings and should settle within three to four days. If the discharge persists, is abundant, has an odor, or if you experience any pain or itching, you should reach out to the hospital.
• Your ear canal will contain dressing/packing that will be taken out during your initial follow-up appointment, which is typically four weeks after your surgery. Due to this packing, your hearing may appear to be worse than it was prior to your operation. We will not be able to evaluate your hearing until this packing is removed from your ear. The definitive outcome regarding your hearing will only be known three months post-surgery, after all healing has occurred.
• If a portion of the packing comes out, it is advisable to cut the loose end of the packing with scissors and keep the remainder in position.
• You must keep your ear dry for the initial few weeks following surgery. Use a cotton wool ball smeared with Vaseline to plug it during showers. It is suggested that you refrain from washing your hair until the ear packing is taken out in the clinic. You may use dry shampoo as an alternative.
• Refrain from straining or lifting heavy objects for the initial few weeks after surgery.
• Blow your nose only gently.
• Steer clear of air travel for two months.
• It is recommended to avoid diving or flying when you are experiencing a cold, if at all possible.
Will I have a follow-up appointment?
You will get an appointment to come back to the clinic four weeks after your surgery. This is primarily to take out the packing and examine your ear.
We will see you again three months post-surgery, during which we will assess your ear and conduct an audiogram; any additional treatments that you may require will be addressed then.
You will need to return to the ENT Department for your follow-up, for at least five years following your surgery. The appointments are typically scheduled annually, and your surgeon may also request an MRI scan to evaluate your ear, usually one year after your surgery. Additional MRI scans may be necessary.
FOR INFORMATION IN GREAT DETAIL ON Cavity problems after mastoid surgery and it’s management PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Mastoid surgery complications PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Mastoid surgery aftercare PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Mastoiditis surgery cost in India PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Ear canal wall up mastoid surgery PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Dizziness after mastoid surgery PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Postoperative advice for mastoid surgery PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Radical mastoid surgery PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Mastoidectomy with Tympanoplasty Surgery -Restoring Ear Health PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Mastoidectomy Surgery: Benefits, Risks, and Recovery PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
What if I have any problems or concerns?
If any patient of ENT requires any surgery, opd consultation or online consultation in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may contact him at the following address-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road ,Ambad ,1 km from Pathardi phata Nashik ,422010 ,Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cel no- 7387590194 , 9892596635


