
Ocular Rhinosporidiosis-various aspects-
Introduction
The eukaryotic unicellular pathogen Rhinosporidium seeberi, a unique organism of the animal-fungal boundary, causes rhinosporidiosis, a persistent, benign, granulomatous infection of the mucosal lining. It has an impact on people of all ages, from youngsters to adults. The nasal mucosa is the most frequent location of infection, followed by the eyes (around 10–15%). India reported the first instance of conjunctival rhinosporidiosis in 1912. The lacrimal sac is the second most common ocular location for infection, after the conjunctiva. It is transmitted by autoinoculation from injured nasal mucosa to other locations, such as the lacrimal sac and conjunctiva.

The most typical sign of ocular rhinosporidiosis is a polyplike (jelly-like) mass on the palpebral conjunctiva. It might also appear like a diverticulum of the lacrimal sac, recurring meibomian gland polyps, gelatinous conjunctival cysts, persistent follicular conjunctivitis in contact lens wearers, peripheral corneal infiltrations, scleral melting, staphyloma, or a tumor of the eyelid or surrounding skin. Mechanical ectropion can result from huge conjunctival lesions. A symptom of rhinosporidiosis of the lacrimal sac might be tears that are tinged with blood.
Report of a Case
After being sent from the ENT OPD with a painless, reddish-pink, fleshy mass on the white part of the right eye, a 25-year-old man from a rural community came to the Ophthalmology OPD of RIO, RIMS Ranchi. For a similar-looking mass inside his right nostril, he had previously visited the ENT OPD. When asked about the order of events, he described the history of an unidentified particle entering his right eye and nose as he was watering the paddy fields, causing the lesion to form in those areas four to five days later. None of his relatives had comparable lesions, and there was no prior record of them.
If Any Patient of ENT Requires Any Surgery, Opd Consultation Or Online Consultation In Clinic of ENT Specialist Doctor Dr. Sagar Rajkuwar ,He May Contact Him At The Following Address-
Prabha ENT Clinic, Plot no 345,Saigram Colony, Opposite Indoline Furniture Ambad Link Road ,Ambad ,1 km From Pathardi Phata Nashik ,422010 ,Maharashtra, India-Dr. Sagar Rajkuwar (MS-ENT), Cell No- 7387590194, 9892596635
He had a fleshy, red mass that was approximately 6 × 12 mm in size when he was inspected. About 2.5 mm from the corneal limbus, on the right eye’s bulbar conjunctiva, supero-nasal to the cornea, was the jelly-like reddish mass. The surface was elevated, and vessels grew into it, but touching it didn’t cause it to bleed. The lesion’s surface had little whitish, round, or oval patches. There was no conjunctival congestion, itching, or discharge.
After a tentative diagnosis of rhinosporidiosis and clinical exclusion of all other potential differential diagnoses, the patient was treated for three months with tablet Dapsone (100 mg BD), and the conjunctival lesion was surgically removed under local anaesthetic, followed by cauterization of the base. For histopathologic analysis, the removed mass was sent. He also received systemic antibiotics (Amoxy-Clav 625mg BD for 5 days) and topical Moxifloxacin (0.5% w/v) eye drops for 2 weeks as postoperative preventative therapy.
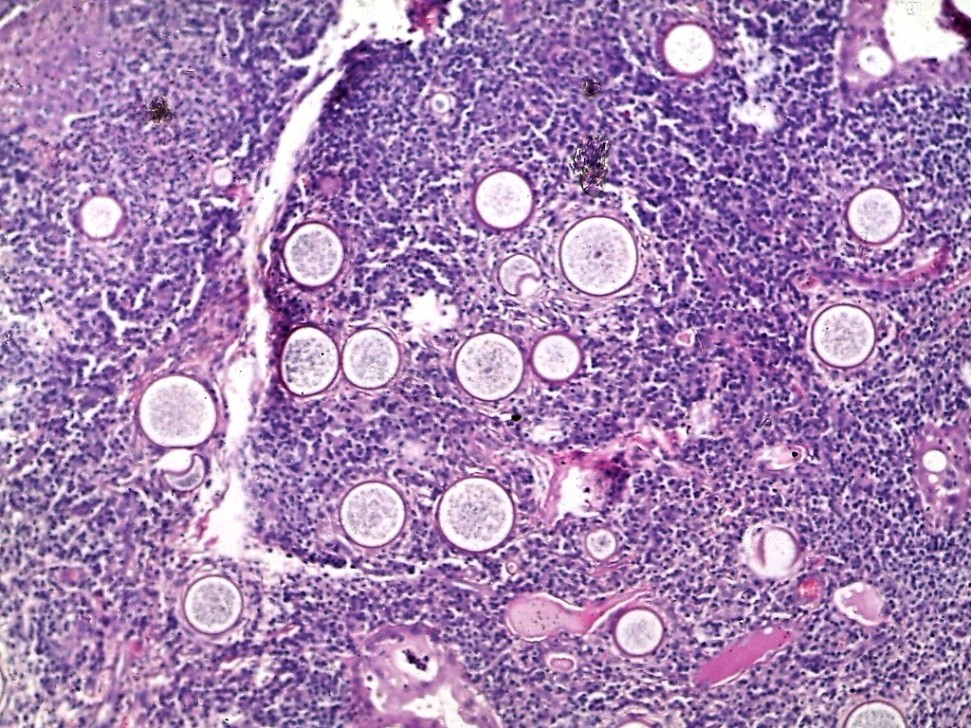
In the bulbar conjunctival tissue of the right eye, HPE discovered minor epithelial hyperplasia and several sporangia in various stages of development and regeneration. Around the sporangia were inflammatory cells, such neutrophils, lymphocytes, plasma cells, and multinucleated giant cells. The thick walls of the sporangia at different stages of the life cycle were highlighted by the periodic acid-Schiff (PAS) stain. Mature sporangia exhibited a surface pore with the release of spores. The results were in line with conjunctival rhinosporidiosis.

Initially, the patient received routine follow-up every 15 days for up to 2 months, then once a month for up to 6 months, and finally once a year. In six months, there was no return of any eye or nasal lesions.
For Update On Further Important Health Related Topics And Frequently Asked Questions On Health Topics By General Population Please Click On The Link Given Below To Join Our WhatsApp Group –
https://chat.whatsapp.com/Lv3NbcguOBS5ow6X9DpMMA
After 45 days after the procedure, the surgical wound on the right eye’s bulbar conjunctiva had fully recovered, and there were no lingering scars.
Discussion
Despite being an infectious illness, little is known about how rhinosporidiosis spreads. Transmission from human to human or animal to human is extremely rare. It is assumed that trauma or interaction with standing water, where spores from soil or water come into touch with the mucosal surface, is the mode of transmission.
The diagnosis is confirmed by an excision biopsy of the lesion, which is followed by histopathology, which reveals sporangia at various stages of development. Although systemic medications, particularly dapsone or Amphotericin-B, may be taken into consideration, their effectiveness is still uncertain. According to the literature, the function of topical antibiotics and antifungals in these instances is not well established. In our instance, the conjunctival lesion was removed and cauterized, and then topical and systemic antibiotics were administered for a short period of time as a post-operative prophylaxis. The conjunctiva and lacrimal sac have comparatively low recurrence rates.
DISCLAIMER-Some patients go to net and directly take treatment from there which can lead to catastrophic consequences-Then- Many people ask then why to read all this text -the reason is that it helps you to understand the pathology better ,you can cooperate with treatment better ,your treating physician is already busy with his patients and he does not have sufficient time to explain you all the things right from ABCD ,so it is always better to have some knowledge of the disease /disorder you are suffering from.
Among the diseases that must be ruled out in the differential diagnosis of ocular rhinosporidiosis are the following:
granuloma caused by pus
Papilloma squamous
adenoma sebaceous
carcinoma of the sebaceous glands
carcinoma of the squamous cells
Cyst in the conjunctiva
An inflamed pingecula
Conjunctival rhinosporidiosis may be clinically distinguished from other lesions that resemble it by a thorough clinical history and careful examination, even if the lesions appear nearly identical to the naked eye. The nasal limbus is the most frequent place where pingecula occurs, but it can also be seen on the temporal side. There is often a long history of exposure to sunshine. Squamous carcinomas are often multifactorial and typically appear later in life. The lesion may bleed upon palpation, and the growth may be rapid. The diagnosis is confirmed by an HPE of the lesion. The finger-like appearance of squamous papilloma, which is strongly linked to HPV infection (associated with cutaneous warts), is confirmed by conjunctival impression cytology. Rhinosporidiosis may resemble a conjunctival cyst, but a thorough examination will reveal that it has a distinct texture and is filled with either blood-mixed or clear fluid. In addition, unlike rhinosporidiosis, there will be no white patches visible on its surface.
In summary
Conjunctival rhinosporidiosis is characterized by a distinctive presentation and a common history of contact with plant matter. The patient was treated according to the standard of care, which included surgical removal with cauterization of the lesion’s base, both in the nasal mucosa and conjunctiva. The diagnosis was verified via a histopathological investigation. Six months after the procedure, the lesion did not reappear
FOR FURTHER INFORMATION IN GREAT DETAIL ON Rhinosporidiosis PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Rhinosporidiosis Pathology Outline PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Rhinosporidiosis Treatment PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Rhinosporidiosis Symptoms PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
FOR FURTHER INFORMATION IN GREAT DETAIL ON Rhinosporidiosis Histology PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
FOR FURTHER INFORMATION IN GREAT DETAIL ON Rhinosporidiosis Life Cycle PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
FOR FURTHER INFORMATION IN GREAT DETAIL ON Rhinoscleroma vs Rhinosporidiosis PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION.
If any patient has any ENT -Ear nose throat problems and requires any , consultation ,online consultation ,or surgery in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may TAKE APPOINTMENT BY CLICKING ON THE LINK GIVEN BELOW-
Clinic address of ENT SPECIALIST doctor Dr Sagar Rajkuwar-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road ,Ambad ,1 km from Pathardi phata Nashik ,422010 ,Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cel no- 7387590194 , 9892596635


