
Treatment Of Chronic Otitis Media -various aspects-
Before understanding Treatment Of Chronic Otitis Media it is necessary to go through a brief introduction of Chronic otitis media. Introduction of Chronic otitis media- It is a suppurative perforation of the tympanic membrane that lasts longer than six weeks and is consistently draining. The symptoms include conductivity-induced hearing loss and otorrhea without discomfort. Complications include the development of cholesteatoma, infections, and auditory polyps. The granulation tissue must be carefully removed, the ear canal must be completely cleaned numerous times daily, and topical corticosteroids and antibiotics must be used. Only the most serious conditions necessitate surgery and systemic antibiotics.

Persistent otitis media in relation to Treatment Of Chronic Otitis Media-
Chronic otitis media can be brought on by acute otitis media, eustachian tube obstruction, mechanical trauma, thermal or chemical burns, blast injuries, or iatrogenic causes. Chronic Otitis, such as following the insertion of a tympanostomy tube. Patients who have craniofacial defects such DiGeorge syndrome, Velocardiofacial syndrome, Shprintzen syndrome, or Shprintzen-Goldberg syndrome are also more vulnerable. Examples include cleft lip and/or palate, 22q11.2 deletion, Down syndrome, and cri du chat syndrome.
Although viruses are the most common cause of otitis media in children, bacteria also frequently affect those children who have chronic suppurative otitis media. The normal aetiology is polymicrobial. Understanding eitiology is necessary as a part of Treatment Of Chronic Otitis Media .The most common bacterium found in this condition (MRSA) is Staphylococcus aureus. Pseudomonas aeruginosa, Proteus species, Klebsiella species, Bacteroides species, and Fusobacterium species are additional infections that can cause the illness. Less frequently, but more frequently, Aspergillus and Candida species are found in immunocompromised individuals. [4] Chronic otitis media as a result of tuberculosis is more typical in areas with a high tuberculosis incidence.
1. Antibiotics as a part of Treatment Of Chronic Otitis Media-
2. Ear Drops as a part of Treatment Of Chronic Otitis Media-
3. Surgery as a part of Treatment Of Chronic Otitis Media-
4. Hearing Aids
5. Vestibular Rehabilitation
6. Prevention versus
Chronic suppurative otitis media (CSOM), which is typified by recurring or prolonged acute otitis media episodes lasting longer than 12 weeks, can damage and perforate the tympanic membrane (TM), which will not heal. CSOM is the most common infectious disease that affects kids worldwide. Risk factors include having Native American, Native Alaskan, or Aboriginal Australian ancestry, poor nutrition, unsanitary living circumstances, family history, low birth weight, cranial abnormalities, and upper respiratory infections. Hearing loss and otorrhoea that enters the external ear canal through the TM perforation are symptoms of CSOM. Even though the average hearing loss is just 10 to 20 dB, there is a chance that it could get worse with severe perforations. Ossicular chain deterioration, which can have a more profound effect on the audiology, can also occur in other circumstances. (50 to 70dB). In these situations, it’s crucial to rule out the possibility of cholesteatoma. Tympanic membrane perforations are possible in the pars tensa as well as the pars flaccida. (albeit the former is overwhelmingly more prevalent). The hole can alternatively be categorised as marginal, central, moist, or dry depending on where it is in respect to the annulus. (respectively, chronic otorrhoea or no otorrhoea in progress).
A subtype of the illness is called CSOM with cholesteatoma. Tympanoplasty and mastoid surgery are necessary for cholesteotoma-as a part of Treatment Of Chronic Otitis Media- The most common cause of middle ear cholesteatomas is an acquired illness condition. They are comprised of a sac of squamous epithelium, which originates at the pars falccida of the TM and frequently grows in the attic. These sacs may protrude from the TM, causing bone to erode and ossicular chains to disintegrate.The same CSOM symptoms and signs, such as foul-smelling otorrhoea, hearing loss, TM perforation, and attic retraction, can also be present with cholesteroleatoma.
A perforated TM is surgically repaired with a tympanoplasty in an effort to prevent reinfection and restore hearing, with or without repairing the ossicles (ossiculoplasty). Although CSOM is the most common indication, mastoidectomy with TM reconstruction may be required in cases of extensive, invasive cholesteatomas. Wullstein and Zollner, who popularised the use of overlay grafts to patch perforated TMs and restore the middle ear’s sound-conduction mechanism, performed the first tympanoplasty treatments in the 1950s as a part of Treatment Of Chronic Otitis Media .Since then, tympanoplasty surgical methods have changed, as this page explains.
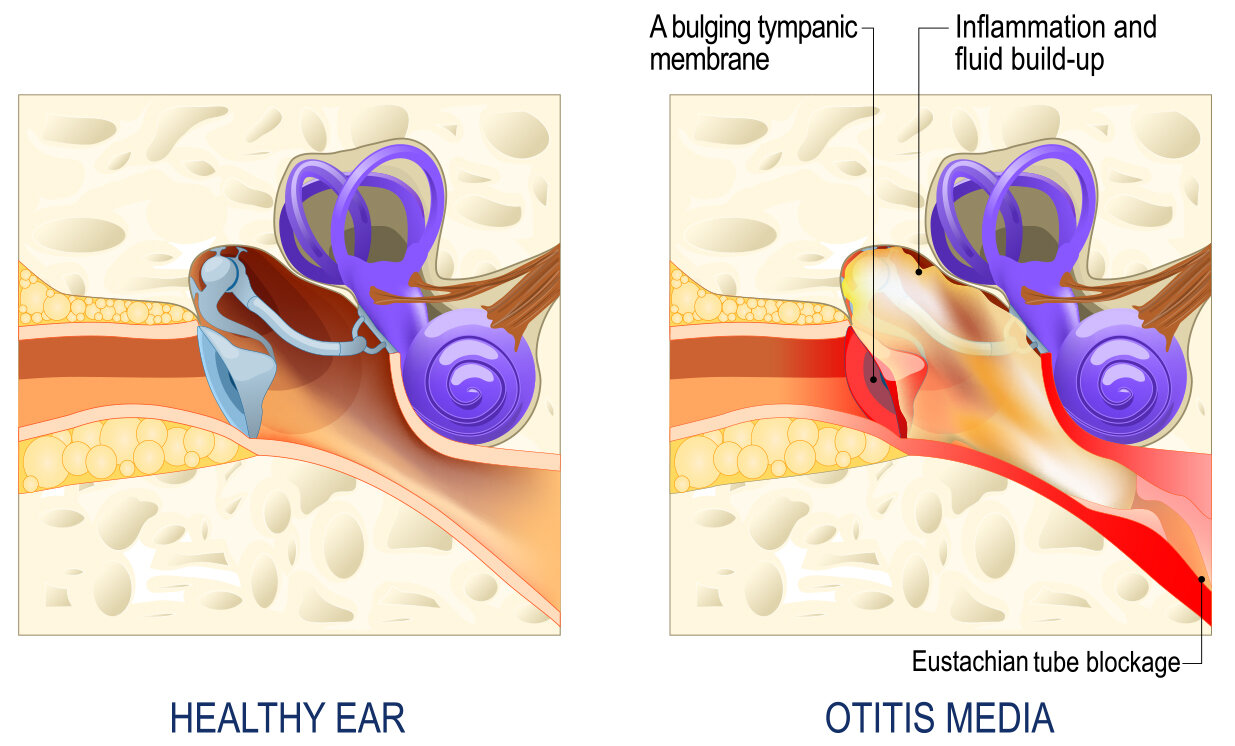
Chronic otitis media with effusion (OME), often referred to as “glue ear,” is a condition in which fluid persists in the middle ear for a long time (more than three months) without evidence of an active infection. It is a prevalent childhood condition that can lead to hearing loss and, if left untreated, might have an impact on the development of speech and language.
Important features of persistent OME:
accumulation of fluids:
The accumulation of non-purulent (non-infected) fluid behind the eardrum in the middle ear space is referred to as otitis media with effusion (OME).
No active infection:
Chronic OME, in contrast to acute otitis media, does not manifest active indications of infection such as pain, fever, or pus discharge.
hearing loss:
Conductive hearing loss can result from the middle ear fluid’s ability to absorb sound vibrations.
Prevalence:
Most children experience at least one bout of OME, which is quite frequent in childhood.
Length:
Fluid that lasts for more than three months is considered chronic OME.
possible difficulties:
Chronic OME, if left untreated, can result in speech and language delays, particularly in young children.

Possible reasons for persistent OME:
Eustachian tube dysfunction:
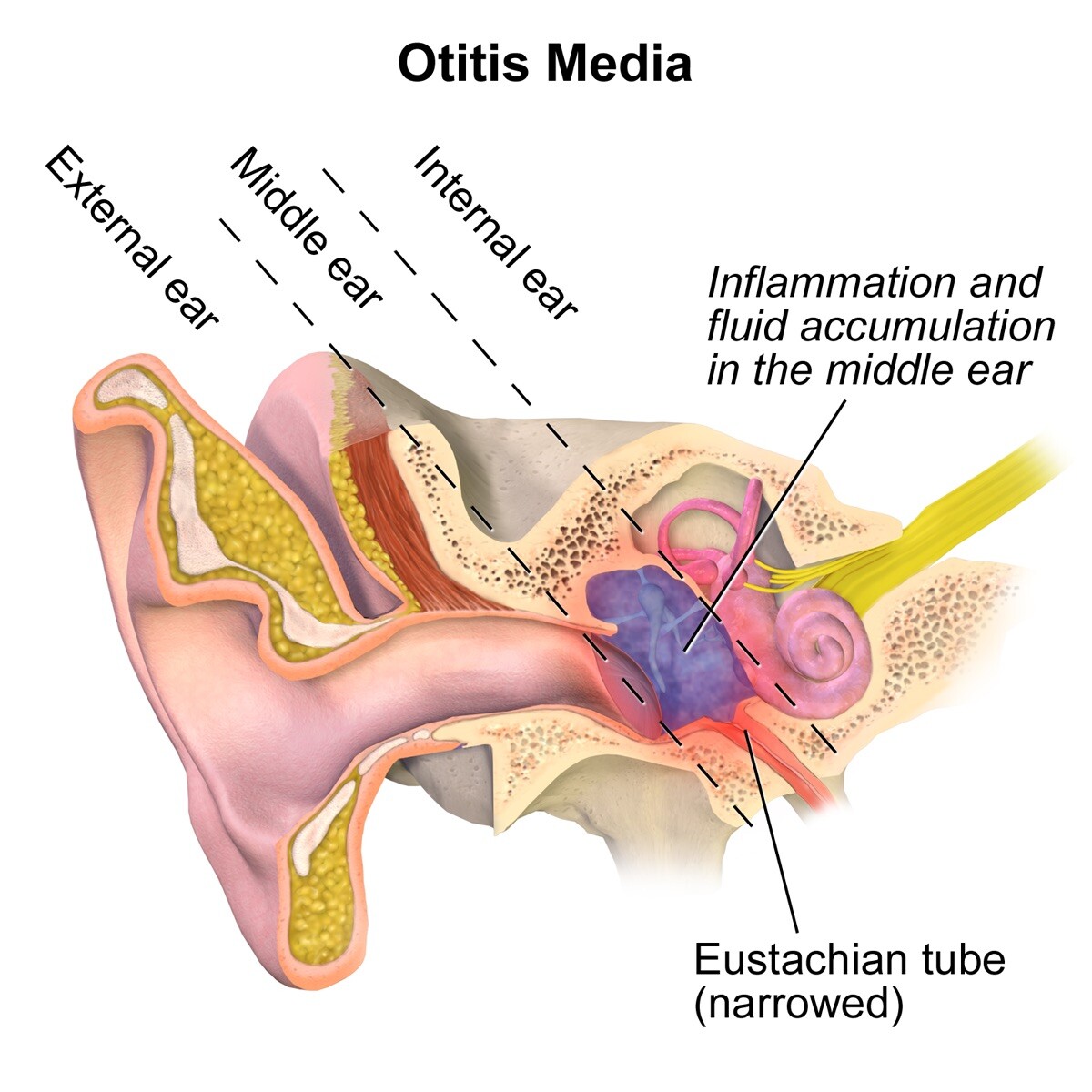
The middle ear is connected to the back of the throat by the Eustachian tube, which aids in fluid drainage and pressure control. Fluid accumulation can result from issues with this tube.
Allergies:
Inflammation and edema in the Eustachian tube and middle ear caused by allergies can lead to OME.
Infections of the upper respiratory tract:
Fluid accumulation may result from the Eustachian tube being inflamed by colds and other respiratory infections.
Palate cleft:
Due to Eustachian tube problems, youngsters with cleft palate have a higher risk.
Adenoids that are enlarged:
The Eustachian tube opening might be blocked by enlarged adenoids, resulting in fluid buildup.
Conclusion:
- Pneumatic otoscopy: A straightforward examination in which the doctor softly blows air into the ear canal to evaluate the movement of the eardrum.
- Tympanometry: A test that evaluates how the eardrum moves in reaction to variations in air pressure.
- Hearing test: The degree and kind of hearing loss are measured using audiometry.
Treatment:
Observation:
Often, OME goes away by itself.
Drugs:
Although decongestants, antihistamines, and corticosteroids can be used, their efficacy is restricted.
ear tubes, tympanostomy tubes
To ventilate the middle ear and drain fluid, little tubes are surgically inserted into the eardrum.
Adenoidectomy:
The adenoids, which are lymphatic tissue located behind the throat, may occasionally need to be removed, particularly if they are big.
Expectation:
- The majority of OME cases heal without any long-term consequences.
- Early diagnosis and treatment can reduce the likelihood of language and speech problems.
Otitis media with effusion
Glue ear; Silent ear infection; Silent otitis media; Serous otitis media; Secretory otitis media; OME
Thick or sticky fluid behind the eardrum in the middle ear is known as otitis media with effusion (OME). It doesn’t happen when you have an ear infection.
Causes
The inside of the ear is connected to the rear of the throat via the Eustachian tube. The purpose of this tube is to aid in fluid drainage and prevent fluid accumulation in the ear. The liquid is consumed after it drains from the tube.
In two ways, ear infections and OME are related:
- Fluid (an effusion) remains in the middle ear for a few days or weeks following the majority of ear infection treatments.
- Fluid accumulates in the middle ear when the Eustachian tube is partially blocked. The ear’s bacteria become trapped and start to multiply. An ear infection may result from this.
The lining of the Eustachian tube may swell, resulting in an increase in fluid in the middle ear, for any of the following reasons:
- Allergies
- Irritants (especially cigarette smoke)
- Infections of the respiratory system
The Eustachian tube may close or become blocked due to the following reasons:
- Drinking while reclining on your back
- Rapid changes in air pressure, such as when going down a mountain route or in an aircraft.
- Any edema within the nose or throat (which in adolescents and adults may include tumors)
Water entering a baby’s ears won’t result in an obstructed Eustachian tube.
Although it can happen at any time of the year, OME is more prevalent in the winter or early spring. It can affect individuals of all ages. It happens most frequently in children under two years old, although it is uncommon in neonates.
There are a few reasons why younger children have OME more frequently than older children or adults:
- Bacteria find it simpler to enter the Eustachian tube since it is shorter, more horizontal, and straighter.
- The Eustachian tube is more floppy and has a smaller, more easily blocked opening.
Because it takes time for the immune system to learn how to identify and fight against cold viruses, young children are more susceptible to colds.
The fluid in OME is typically thin and watery. It was formerly believed that the fluid became thicker with time in the ear. (Thick fluid in the middle ear is sometimes referred to as “glue ear.”) However, it is now understood that the fluid’s thickness is determined by the ear itself, not by how long the fluid is there.
Symptoms
Children with OME don’t behave as though they have an ear infection.
Frequently, the signs of OME are not apparent.
Older children and adults frequently report muffled hearing or a feeling of fullness in the ear. Hearing loss can lead to young children raising the volume of the television.
Tests and examinations
Following treatment for an ear infection, the healthcare professional may discover OME when examining your child’s ears.
The provider will inspect the eardrum for particular alterations, such as:
- Air bubbles on the surface of the eardrum
- When using a light, the eardrum is dull.
- A tympanic membrane that appears unresponsive when small puffs of air are blown at it
- Fluid behind the eardrum
The tympanometry test is a reliable method for identifying OME. The quantity and thickness of the fluid may be determined with the use of this test’s findings.
With: The fluid in the middle ear can be precisely detected.
- Otoscope for sound
- Reflectometer – a portable gadget
Formal hearing testing may be conducted using an audiometer or another method. The provider may be able to make treatment decisions with this information.
Therapy
Unless there are additional signs of an infection, most providers won’t initially address OME in youngsters. They will, however, examine the issue again in two to three months.
The following modifications can be made to assist in clearing the fluid behind the eardrum:
- Keep away from cigarette smoke
- Promote breastfeeding for infants
- Avoid triggers (like dust) to treat allergies. Allergy medications are available for adults and older children.
The liquid will usually clear up by itself. Before recommending treatment, your child’s provider may advise observing the illness for a period of time to determine whether it is getting worse.
The provider may suggest the following if the fluid is still there after six weeks:
- Still observing the issue
- An auditory examination
- A single course of antibiotics, if they weren’t administered sooner.
Antibiotics may be tested in a youngster if the fluid persists for eight to twelve weeks. These medications are not always effective. A further test is necessary for teenagers and adults at this time to look for a tumor in the nose or throat.
The youngster should have their hearing tested at some point. Antibiotics or ear tubes may be necessary if there is considerable hearing loss (above 20 decibels).
Even if there is no significant hearing loss, tubes are likely necessary if the fluid persists for 4 to 6 months.
In some cases, the Eustachian tube cannot function correctly unless the adenoids are removed.
If any patient requires treatment for chronic otitis media, he may consult ENT specialist doctor Dr Sagar Rajkuwar (MS-ENT) at the following adress-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture, Ambad link road ,Ambad ,1 km from Pathardi phata Nashik 422010 ,Maharashtra ,India-Dr Sagar Rajkuwar (MS-ENT), Cel no- 7387590194, 9892596635


