
Lingual tonsillectomy-various aspects-
A lingual tonsillectomy is a surgical operation aimed at removing excessive tissue or decreasing the size of the tongue to enhance breathing during sleep. It is carried out inside the mouth, with no external cuts required.
A lingual tonsillectomy is utilized to address:-

Obstructive sleep apnea-
Lingual tonsil hypertrophy can result in obstructive sleep apnea, and a lingual tonsillectomy can provide assistance.
In case if you are suffering from obstructive sleep apnoea ,you need to consult a qualified and experienced ENT specialist doctor or a Chest physician/Pulmonologist.
If Any Patient of ENT Requires Any Surgery, Opd Consultation Or Online Consultation In Clinic of ENT Specialist Doctor Dr. Sagar Rajkuwar ,He May Contact Him At The Following Address-
Prabha ENT Clinic, Plot no 345,Saigram Colony, Opposite Indoline Furniture Ambad Link Road ,Ambad ,1 km From Pathardi Phata Nashik ,422010 ,Maharashtra, India-Dr. Sagar Rajkuwar (MS-ENT), Cell No- 7387590194, 9892596635
Briefly speaking if a patient of obstructive sleep apnoea is suffering from overweight ,he is advised to reduce his weight ,his sinus problems ,deviated nasal septum problems are evaluated ,only if he is symptomatic his CTSCAN-PNS is done, history of smoking ,tabaco consumption is evaluated ,his direct laryngoscopy is done. A test called video MRI is done when the patient is in state of sound sleep- which directly indicates the site of obstruction.

Lingual tonsillitis-
Lingual tonsillectomy serves as a remedy for inflammatory lesions of the lingual tonsil, but it is infrequently executed due to the low incidence of diagnosed lingual tonsillitis.
During the operation, a Lindholm laryngoscope is utilized to reveal the base of the tongue, and a CO2 laser or suction debrider is employed to ablate the lingual tonsils.
Post-surgery, you can anticipate remaining in the hospital for 1–2 days. You will need to ensure that you can breathe freely, experience no bleeding, and consume adequate fluids. It is advisable to have someone stay with you for safety at home on the first night.
Following the procedure, you may notice a suture in your mouth, but it will dissolve over the course of two weeks. There will be no need for any particular wound care.
A lingual tonsillectomy has minimal impact on your voice since the front part of your tongue remains functional for speech.
a remedy for inflammatory lesions of the lingual tonsil –
Lingual tonsillectomy is a surgical intervention that is rarely performed as lingual tonsillitis is seldom diagnosed.
Lingual tonsillectomy is a surgical procedure that is rarely conducted since lingual tonsillitis is not commonly identified. We have examined a cohort of patients suffering from lingual tonsillitis or lingual tonsil hyperplasia who underwent lingual tonsillectomy. The discussion covers lingual tonsil lesions, the anatomy and histology of the lingual tonsil, and the surgical methods utilized for lingual tonsillectomy.
The posterior part of the tongue also has lymphoid tissue (tonsils) which, when swollen, can obstruct airflow. The surgical excision of tongue base tissue results in an enhancement of the airway volume in the region located behind the tongue.
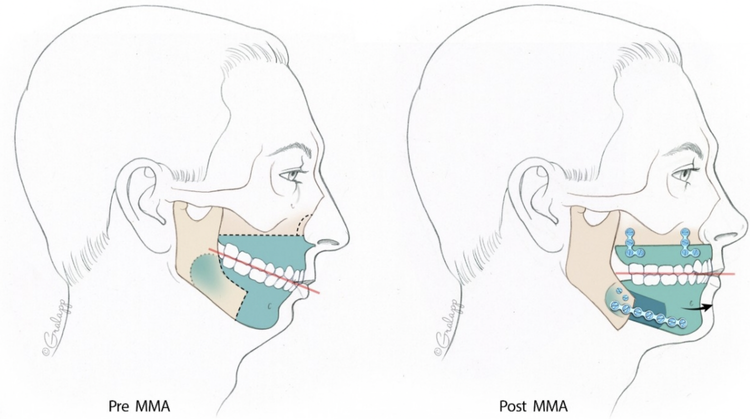
Genioglossus Advancement
A surgical operation where the muscle of the tongue connected to the lower jaw is moved forward, creating a firmer and less collapsible tongue during sleeping. In this operation, a small opening in the bone is created in the lower jaw, and the segment of bone along with the tongue‘s attachment is pulled forward and secured by a small screw or a plate on the outer surface of the bone.
Is lingual tonsillectomy dangerous ?
Lingual tonsillectomy is a secure and established technique to decrease the size of enlarged lingual tonsils. Complications are quite uncommon .In case there is bleeding in hospital post-op it can be controlled by the operating ENT surgeon .
For update on further important health related topics and frequently asked questions on health topics by general population please click on the link given below to join our WhatsApp group –
https://chat.whatsapp.com/Lv3NbcguOBS5ow6X9DpMMA
Lingual tonsillectomy vs tonsillectomy-FOR THIS PL CLICK ON THE LINK GIVEN BELOW-FOR TONSILLECTOMY IN GREAT DETAIL-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION .
If you are suffering from obstructive sleep apnoea and require consultation from ENT specialist doctor ,pl click on the link given below-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION .
www.entspecialistinnashik.com
Tonsillectomy is frequently accompanied by adenoidectomy surgery in paediatric population ,for DETAILS OF ADENOIDECTOMY SURGERY PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION .
Obstructive sleep apnea

Obstructive sleep apnea is the most prevalent sleep-related breathing disorder. Individuals with obstructive sleep apnea frequently cease and resume breathing while they are asleep.
There are various forms of sleep apnea. Obstructive sleep apnea takes place when the muscles in the throat relax and obstruct the airway. This occurs intermittently many times throughout sleep. A symptom of obstructive sleep apnea is snoring.
There are treatments available for obstructive sleep apnea. One treatment involves a device that applies positive pressure to maintain the airway open during slumber. Another alternative is a mouthpiece that pushes the lower jaw forward while sleeping. For some individuals, surgery might also be a viable option.
Obstructive sleep apnea is a disorder in which sleep is disrupted by irregular breathing. In sleep apnea, the flow of air is hindered due to the airway obstructing it. These disruptions last for more than 10 seconds and occur at least 5 times per hour during your sleep duration.
Genioglossus advancement
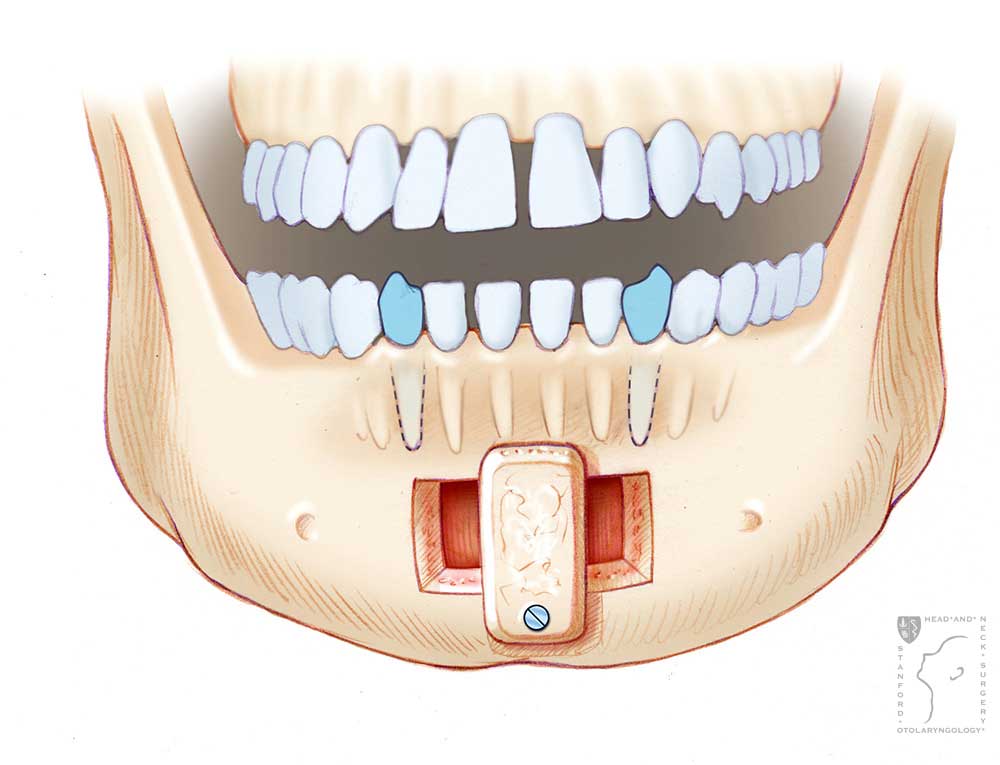
Genioglossus advancement is significant in the toolkit of the obstructive sleep apnea surgeon and has evolved through numerous variations over the years. A newly articulated method involves performing a box osteotomy, which extends along the lower edge of the mandible to enhance the activation of the suprahyoid muscles. Here we present an additional refinement of the procedure that utilizes virtual planning to enhance the safety and precision of genial tubercle retrieval. Furthermore, the angling of the lateral osteotomies improves the contact between bone surfaces. Prior to the osteotomy, the surgeon can drill into the buccal plate to lessen the chin’s profile. This technique is especially beneficial for patients who are prognathic initially or those who become prognathic following simultaneous maxillomandibular advancement. Here we explore this distinctive method, illustrating how the patient’s profile may be harmonized even as the genial tubercle is advanced.
Moderate to severe obstructive sleep apnea (OSA) is extremely prevalent, impacting an estimated 425 million adults. Although positive airway pressure is the primary treatment, many are unable to tolerate positive airway pressure and consider surgical options such as genioglossus muscle advancement (GA). This surgery involves advancing the genioglossus muscle, enhancing tension at the base of the tongue, and reducing the likelihood of tongue prolapse into the airway during sleep. A recent meta-analysis of GA for the treatment of OSA discovered that this surgery alone can lead to a reduction in apnea-hypopnea index by an average of 41. 7%.
Various methods of GA have been documented, including the rectangular osteotomy, trapezoid osteotomy, elliptical window GA, trephine osteotomy, and mortized genioplasty. The range of techniques highlights the difficulty of predictably advancing the genial tubercle safely and reproducibly. Demian et al. described a rectangular osteotomy that reaches the inferior border of the mandible; after the bone flap is advanced, the osteotomy gap is filled with bone graft.
Here we outline a modified technique that involves en bloc advancement of the mandibular symphysis and capturing the genial tubercle through virtual planning. The genial tubercle is advanced without altering the chin profile. Alternatively, for patients who are prognathic, the chin profile is decreased, but the genial tubercle is advanced simultaneously.
How painful is a lingual tonsillectomy?
Pain associated with a lingual tonsillectomy is reduced compared to a conventional tonsillectomy because the throat muscles remain unexposed. You will be provided with sufficient pain relief medication during the postoperative phase. During your follow-up appointment one week later, your doctor can assist you with any concerns regarding your recovery.
What are the risks of lingual tonsillectomy?
The subsequent video showcases a dialogue regarding Tongue Region procedures, encompassing lingual tonsillectomy:
RISKS.
Hemorrhage. Similar to any surgical intervention, there is a possibility of hemorrhage.
Infection.
Numbness or tingling of the tongue.
Weakness in the tongue or difficulties in swallowing.
Dental injury.
Requirement for further procedures.
FOR INFORMATION IN GREAT DETAIL ON Tonsillectomy diet day by day for child PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Tonsillitis White Stones PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
FOR INFORMATION IN GREAT DETAIL ON Tonsillitis White Patches PL CLICK ON THE LINK GIVEN BELOW-It Is Always Better To View Links From Laptop/Desktop Rather Than Mobile Phone As They May Not Be Seen From Mobile Phone. ,In Case Of Technical Difficulties You Need To Copy Paste This Link In Google Search. In Case If You Are Viewing This Blog From Mobile Phone You Need To Click On The Three Dots On The Right Upper Corner Of Your Mobile Screen And ENABLE DESKTOP VERSION.
Surgery to remove the tonsils is called a tonsillectomy (ton-sih-LEK-tuh-me). The tonsils are two oval-shaped tissue cushions located in the back of the throat. Each side has only one tonsil.
In the past, tonsillectomy was used to treat infection and inflammation of the tonsils. Tonsillitis is the term for this illness. Tonsillectomy is still used for this illness, but only when tonsillitis occurs frequently or when other treatments have failed to improve it. The majority of tonsillectomies performed today are to address respiratory issues that occur while sleeping.
Additionally, tonsillectomy may be used to address breathing and other issues brought about by enlarged tonsils, as well as to address uncommon tonsil illnesses.
It takes ten to fourteen days to recuperate after a tonsillectomy.
The rationale behind it
The following conditions are treated with a tonsillectomy:
- Recurring, persistent, or severe tonsillitis.
- Difficulty breathing while sleeping.
- additional issues brought about by enlarged tonsils.
- Tonsil bleeding.
- Uncommon tonsil disorders.
Tonsillitis
An inflammation of the tonsils is known as tonsillitis. The tonsils are the body’s first line of defense against bacteria and viruses that enter the mouth. The tonsils are made susceptible to inflammation, which is the term for swelling and irritation caused by infection.
However, after adolescence, the tonsil’s immunological activity decreases. Perhaps this is the reason why tonsillitis is so uncommon in adults.
To address recurrent tonsillitis, a tonsillectomy may be recommended by an ENT doctor, who specializes in disorders of the ear, nose, and throat. This is a recurrence of tonsillitis:
- At least seven times during the previous year.
- At least five times each year during the previous two years.
- At least three times a year over the previous three years.
Additionally, the treatment could be recommended by an ENT specialist if:
- Antibiotics are ineffective in treating tonsillitis brought on by a bacterial infection.
- A pus-producing illness behind a tonsil does not respond to treatment or drainage. A tonsillar abscess is the name for the collection of pus.
Complications of enlarged tonsils
Repeated infections can cause the tonsils to grow larger. Or they may just be huge. Problems brought on by enlarged tonsils can be treated with a tonsillectomy, such as:
- Difficulty breathing.
- Obstructive sleep apnea, which causes breathing to cease during sleep.
Other illnesses or disorders of the tonsils
In addition to treating other uncommon illnesses or conditions affecting the tonsils, a tonsillectomy may also be used to treat:
- In one or both tonsils, there is cancer.
- Bleeding from blood vessels close to the surface of the tonsils.
- Halitosis is severe foul breath associated with minute stones that develop in the tonsils. Tonsilloliths or tonsil stones are the names of the stones.
Hazards
Tonsillectomy, like other surgical procedures, carries some dangers, such as:
- Response to anesthesia. Medications used to induce sleep during surgery sometimes result in minor, transient issues. These may include muscle pain, nausea, vomiting, or headache. Serious, long-term issues and mortality are uncommon.
- Swelling. Swelling of the tongue and the soft roof of the mouth, known as the soft palate, can lead to difficulty breathing. This is most likely to occur within the first couple of hours following the surgery.
- Bleeding during the procedure. In rare instances, there is significant bleeding during the operation. A longer hospital stay and therapy are necessary for this.
- Bleeding throughout recovery. Bleeding is possible during the healing process. If the wound’s scab falls off and irritates the skin, this is the most probable outcome.
- Infection. Surgery seldom results in an infection that needs medical care.
How you get ready
The healthcare staff advises you on how to get ready for a tonsillectomy.
Information
Your healthcare staff must be informed about:
- Everything you consume, including dietary supplements and medications. Remember to add the ones you get without a prescription.
- Family or personal history of adverse responses to anesthesia.
- A past history of bleeding problems, either in the family or in the individual.
- Any known allergies or other responses to medications, such as antibiotics.
Direction
You might be asked by your medical staff to:
- Several days before the procedure, either stop taking or modify the dose of certain medications.
- Avoid eating anything after midnight prior to the procedure.
- Be sure to have transportation back home.
- Give yourself 10 to 14 days to recuperate. Adults may need more time than youngsters do.
Before surgery, you or your youngster can require bloodwork or testing.
If your tonsillectomy is for the treatment of obstructive sleep apnea, other airway obstructions, or certain other disorders, you may require a polysomnography, also known as a sleep study.
If Any Patient of ENT Requires Any Surgery, Opd Consultation Or Online Consultation In Clinic of ENT Specialist Doctor Dr. Sagar Rajkuwar ,He May Contact Him At The Following Address-
Prabha ENT Clinic, Plot no 345,Saigram Colony, Opposite Indoline Furniture Ambad Link Road ,Ambad ,1 km From Pathardi Phata Nashik ,422010 ,Maharashtra, India-Dr. Sagar Rajkuwar (MS-ENT), Cell No- 7387590194, 9892596635
Issued in public interest by –
www.entspecialistinnashik.com
-FOR INFORMATION IN GREAT DETAIL What Does a Healing Tonsillectomy Look Like? – Stages, Pictures, and Recovery Guide PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/healing-tonsillectomy/
-FOR INFORMATION IN GREAT DETAIL What Age Is Too Late to Remove Tonsils? Experts Explain PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/what-age-is-too-late-to-remove-tonsils/
-FOR INFORMATION IN GREAT DETAIL Does Removing Tonsils Change Your Voice? Truth Explained by Doctors PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/does-removing-tonsils-change-your-voice/
-FOR INFORMATION IN GREAT DETAIL When Are the Worst Days After Tonsillectomy and Adenoidectomy? Doctor’s Guide PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/what-are-the-worst-days-after-tonsillectomy-and-adenoidectomy/
-FOR INFORMATION IN GREAT DETAIL Can Grade 3 Tonsils Cause Sleep Apnea? Doctor Explains PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/can-grade-3-tonsils-cause-sleep-apnea/
-FOR INFORMATION IN GREAT DETAIL Why Do Tonsillitis White Stones Form? Causes & Easy Fixes PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/tonsillitis-white-stones/
-FOR INFORMATION IN GREAT DETAIL Tonsillitis Removal Surgery PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/tonsillitis-removal-surgery/
-FOR INFORMATION IN GREAT DETAIL Tonsillitis White Patches: Causes, Symptoms, and Treatment Explained PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/tonsillitis-white-patches/
-FOR INFORMATION IN GREAT DETAIL Tonsillitis Surgery: A Guide to Health PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/tonsillitis-surgery/
-FOR INFORMATION IN GREAT DETAIL Tonsillitis Treatment Guide: How to Get Relief Quickly PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/tonsillitis-treatment/
-FOR INFORMATION IN GREAT DETAIL Tonsillitis symptoms PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/tonsillitis-symptoms/
-FOR INFORMATION IN GREAT DETAIL Tonsillectomy diet day by day for child PL CLICK ON THE LINK GIVEN BELOW-It is always better to view links from laptop/desktop rather than mobile phone as they may not be seen from mobile phone. ,in case of technical difficulties you need to copy paste this link in google search. In case if you are viewing this blog from mobile phone you need to click on the three dots on the right upper corner of your mobile screen and ENABLE DESKTOP VERSION-
https://healthuseful.com/tonsillectomy-diet-day-by-day-for-child/


