

How Fast Does Cholesteatoma Grow? ENT Warning Signs You Shouldn’t Ignore
In most cases, cholesteatomas develop slowly, sometimes over months or even years, and may not manifest any symptoms for a long period of time. Induced cholesteatomas often develop faster than those that are present at birth. Different people can have quite different growth rates.
Elaborate:
Slow Growth:
Cholesteatomas are notorious for their gradual growth, which may make them hard to identify in the early stages.
Acquired vs. Congenital:
Cholesteatomas that are present at birth are typically congenital and tend to develop more slowly, usually at a rate of around 1 mm in diameter per year. Cholesteatomas that are acquired and manifest later in life may grow more quickly.
Variation in Growth Rate:
The rate at which cholesteatomas develop might differ greatly from person to person, with some expanding more quickly than others.
Asymptomatic Phase:
Prior to exhibiting obvious symptoms such as hearing loss, ear discharge, or dizziness, many cholesteatomas might go unnoticed for years.
The Value of Early Identification:
Early detection and treatment of cholesteatomas are essential to avoid consequences such hearing loss and harm to the structures of the middle ear, even if their growth is slow.

What constitutes a cholesteatoma?
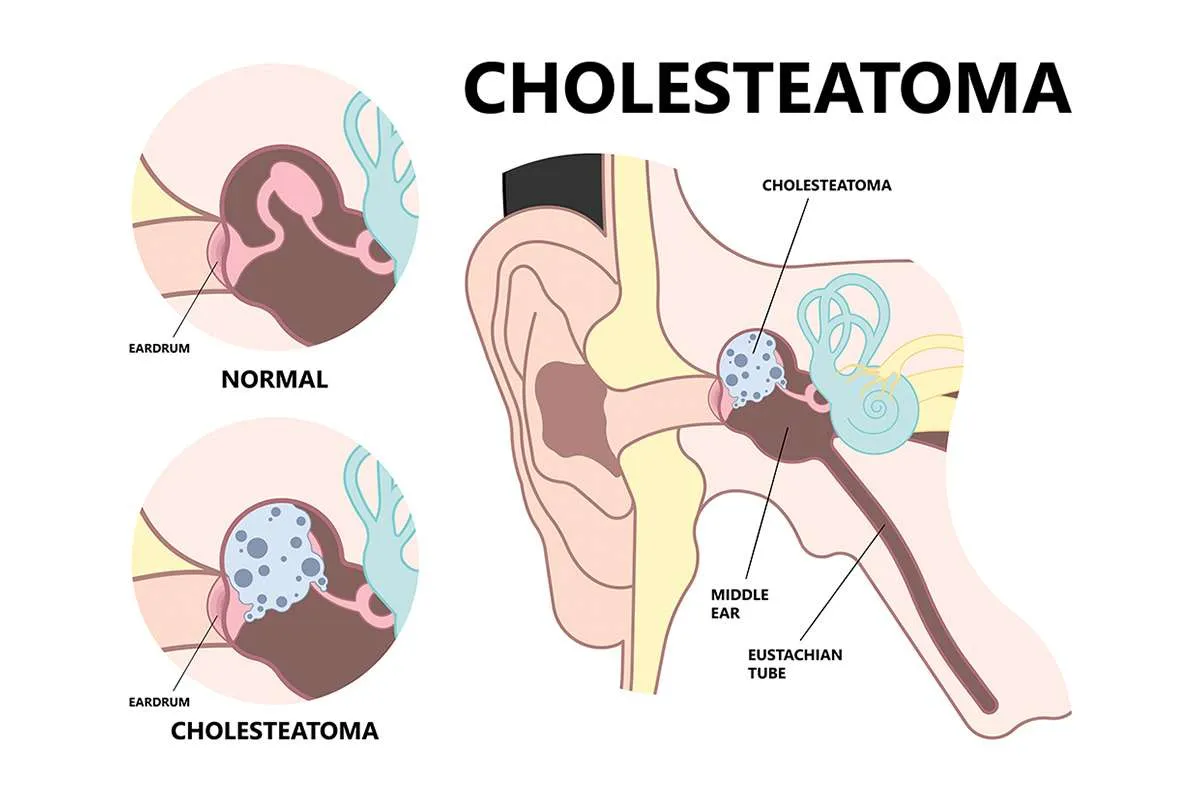
The middle ear is where a cholesteatoma, a benign, aberrant development of skin-like tissue, occurs. Cholesteatomas are uncommon. Although it can be congenital, it most frequently manifests as a consequence of chronic alterations in ear pressure.
Skin cells from the lining of the ear canal seem to get trapped in the middle ear. These skin cells would not ordinarily be found there. Skin cells, such as those that line the ear canal, generally proliferate on a regular basis to replace those that have died. These skin cells typically simply peel off. Over time, this accumulation of dead skin cells can lead to a cholesteatoma if the dead cells become trapped and cluster together.
Although a cholesteatoma is not a kind of cancer, it is nevertheless significant because it may cause severe consequences if left untreated, such as irreversible hearing loss, nerve injury, and potentially deadly infections like meningitis.
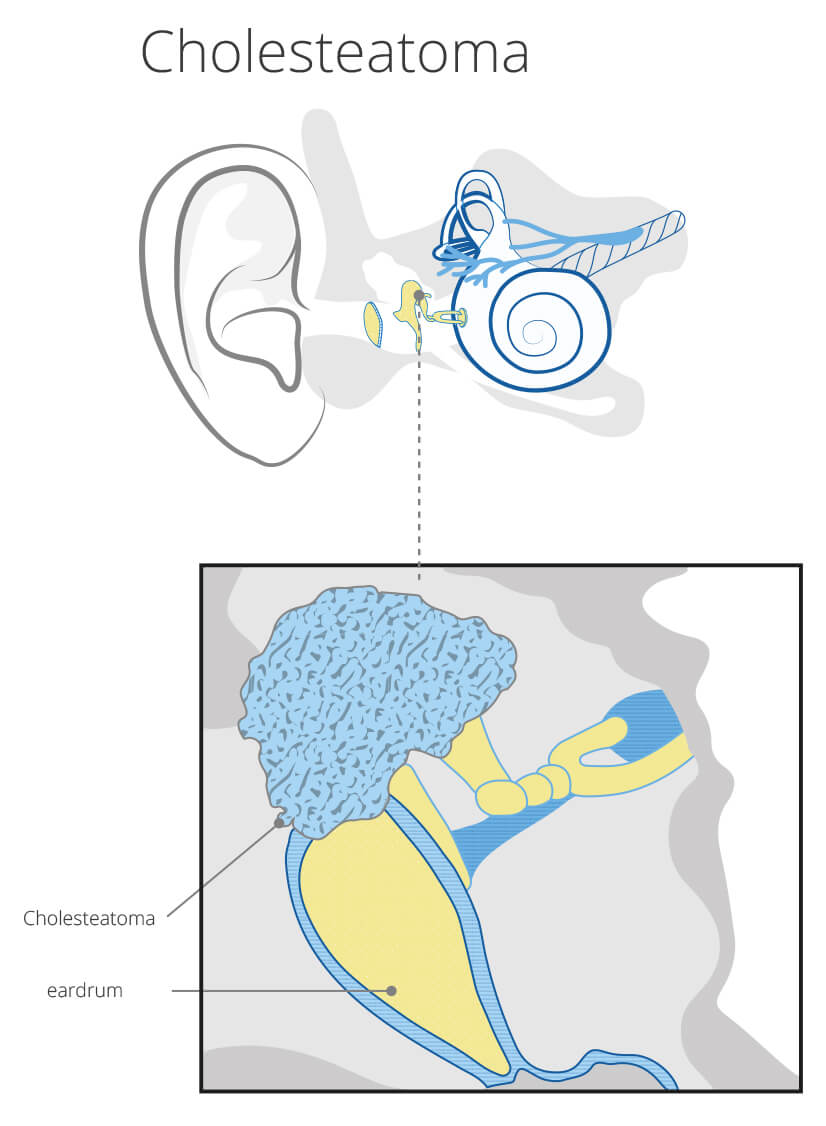
What does a cholesteatoma look like?
The cholesteatoma is the mass of tiny white bumps (white keratin debris) that may be seen on the left-hand side of the close-up picture below.
Is a cholesteatoma dangerous?
Without therapy, the infection will spread farther and farther into the ear, potentially reaching the brain and inner ear, resulting in irreversible hearing loss. It would be quite unusual for it to be that awful in locations with excellent medical facilities, but this might occur in areas with poor healthcare resources.
Cholesteatoma kinds
Cholesteatoma present at birth
This is congenital cholesteatoma. Small skin cells are drawn into the middle ear, obstructing the Eustachian tube, even when the eardrum is healthy.
This then results in persistent fluid in the middle ear (which should normally be fluid-free) and may lead to hearing loss. Between the ages of six months and five years, when the child’s hearing fails to mature, this is evident. This is a very uncommon ailment, and its etiology is unclear.
cholesteatoma acquired
This kind of cholesteatoma usually manifests in adults between the ages of 30 and 50. The reason is still unknown. A cholesteatoma might occasionally develop in an adult following the insertion of a grommet, a small tube inserted through the eardrum as a treatment for middle ear issues, during childhood.
Signs of a cholesteatoma
Because a cholesteatoma grows slowly over many months, an early one may be asymptomatic.
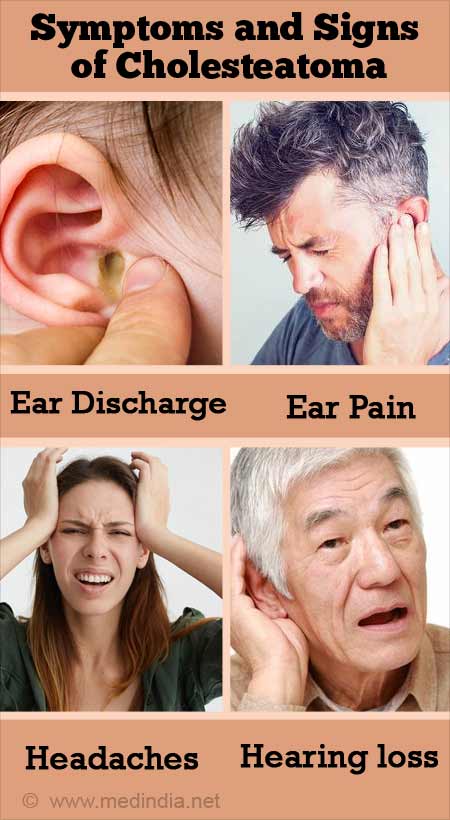
Among other prevalent symptoms are:
Discharge.
loss of hearing.
Dizziness.
The sensation of a full ear.
Release
A discharge from one ear is typically the first sign. Its color is typically a little bit watery, and sometimes it has a yellow or green hue. A doctor examining the ear may notice a slight odor from the discharge, which can resemble an outer ear infection (otitis externa) or an inner ear infection (otitis media) with a perforated eardrum.
It is often treated (incorrectly) with antibiotic ear drops or tablets since it resembles these prevalent infections. Although these therapies may provide some relief, the condition never completely resolves. A cholesteatoma is typically painless.
Hearing loss
Over time, that ear may experience hearing loss. Without therapy, the cholesteatoma might extend into the inner ear’s balance organ, resulting in vertigo or imbalance. A ringing in the ear (tinnitus) may also be present.
Additional signs
In extremely uncommon circumstances, it may eventually infect the brain tissue or the lining of the brain by spreading just adjacent to the brain. Since the cholesteatoma usually grows slowly and most individuals would seek medical treatment if they experience the symptoms described above, this is quite improbable.
The reasons behind a cholesteatoma
We all have skin lining the inside of our ear canals. It is a regular component of our ear and is designed to be there. In exceptional cases, however, a cholesteatoma can occur when the skin immediately adjacent to the eardrum, located deep within the ear, is slowly drawn into the middle ear, where it does not belong.
The cause of this is unknown, but it is often linked to the eardrum being retracted, or drawn inward, further than it should be.
Over the course of several months, this skin then develops into a little pearl, or ball, that continues to tunnel its way farther into the ear. It causes harm to the fragile bones within the middle ear, which are essential for hearing. It’s now painful.
How prevalent are cholesteatomas?
This occurrence is rare. It is thought that a cholesteatoma will be identified in between 7 and 13 people out of every 100,000 members of the population annually, and that the average physician will see a new case every four to five years.
Risk factors for cholesteatoma
Individuals with a history of ear infections are more likely to develop cholesteatoma, which is more prevalent in men than women. Other risk factors include the following:
Prior operation.
Continuous negative pressure in the middle ear, which may lead to the eardrum retracting (‘pulled in’).
Injured ear.
Certain genetic disorders, like Turner syndrome or Down syndrome.
What methods are used to diagnose a cholesteatoma?
The typical symptoms may lead the ear specialist (ENT doctor) or doctor to believe that a cholesteatoma is present. The cholesteatoma may be seen when the ear is inspected with a torch (an otoscope). The tympanic membrane, or eardrum, may also have a hole (perforation) in it.
Since the symptoms manifest gradually and resemble typical ear infections, the diagnosis is frequently delayed.
Because a cholesteatoma typically produces a lot of pus in the ear that obstructs the doctor’s view of the eardrum, it might be challenging for them to detect.
Because of this, a hospital ear expert will often make the diagnosis.
Using a small suction tube, the ear expert will remove the fluid and examine the eardrum thoroughly under a microscope with magnification.
A professional may often see the cholesteatoma pushing through the eardrum by examining it closely.
A professional examination, often a CT scan or an MRI, is then necessary to determine the extent of its spread inside the ear.
Do I require any additional testing?
Deafness or hearing loss might be revealed by hearing tests (audiometry). In a hospital clinic, these tests are often conducted. It’s possible that samples (swabs) of the ear discharge will also be taken. Pseudomonas is a microorganism that is frequently found in the discharge and is the source of the odor.
In order to assess the degree of damage done by the cholesteatoma and make plans for future treatment, a CT scan may be necessary.
If any patient has any ENT -Ear nose throat problems and requires any , consultation ,online consultation ,or surgery in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may TAKE APPOINTMENT BY CLICKING ON THE LINK GIVEN BELOW-
Clinic address of ENT SPECIALIST doctor Dr Sagar Rajkuwar-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road ,Ambad ,1 km from Pathardi phata Nashik ,422010 ,Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cel no- 7387590194 , 9892596635
Treatment for cholesteatomas
Eardrops with antibiotics
Although antibiotic ear drops can kill any infection surrounding the cholesteatoma, they won’t address the underlying issue. Before receiving a cholesteatoma diagnosis, many individuals would have been given antibiotic ear drops without effect.
Surgery
A specialist in ear, nose, and throat surgery (an ENT doctor) performs the surgical procedure, which typically involves surgery under a general anaesthetic. The goals of the procedure are to remove the cholesteatoma and then clear out a portion of the middle ear so that air may flow more freely. With luck, this will prevent the cholesteatoma from recurring.
Depending on the size of the cholesteatoma and the patient’s medical history, a specialized ear physician will recommend the optimal type of cholesteatoma surgery.
A mastoidectomy is a frequent procedure used to remove the cholesteatoma from the bone at the back of the ear, the mastoid, or a ‘combined approach tympanoplasty,’ in which the injured portion of the eardrum is also removed and replaced.
Additional treatment
Regular visits to an ear specialist will be advised to remove any small pieces of wax or debris from deep within the ear if the patient is not a candidate for surgery (for example, if they are extremely old or weak or have other significant medical issues). Although it won’t address the issue, it will prevent it from getting any worse.
Problems associated with a cholesteatoma
A cholesteatoma will gradually grow and spread if left untreated. It is able to eat into (erode) and obliterate anything in its way as it grows.
Potential side effects include:
The minute bones of the ear, known as the ossicles, are damaged and eventually destroyed. Permanent hearing loss can result if these are harmed.
Injury to the mastoid process. This is the dense, bony mass that can be felt behind the ear. The mastoid bone is typically made up of air pockets, similar to a honeycomb. A cholesteatoma, which is a benign tumor, can develop in the mastoid bone, leading to infection and destruction.
injury to the cochlea and other inner ear components. Balance issues, vertigo, or permanent deafness on that side may result from this.
Harm to neighboring nerves that go to the face. As a result, some of the facial muscles may become weak (paralyzed).
Frequently, cholesteatoma becomes infected, and the infection can extend to surrounding areas of the body. In very rare cases, a cholesteatoma may erode the skull and enter the brain next to the ear. Meningitis, brain abscess, and other illnesses can result from the spread of infection. It is possible that these circumstances will result in death.
Please be aware that a cholesteatoma, despite its unpleasant sound, is not malignant (cancerous) and does not spread to other areas of the body.
What do things look like?
The severity of the harm done by the cholesteatoma by the time it is identified and treated determines this. Additionally, it depends on whether any problems, such as meningitis or deafness, have arisen. The earlier the procedure is performed, the greater the possibility of a positive result.
You should be followed up in an ENT clinic if you have ever had a cholesteatoma.
Is it possible for a cholesteatoma to recur?
An MRI scan, not surgery, is used more and more to assess and determine whether a cholesteatoma has reappeared. Additional surgery may be necessary if the ear begins to discharge once more.
Over the course of many months, a cholesteatoma develops slowly.
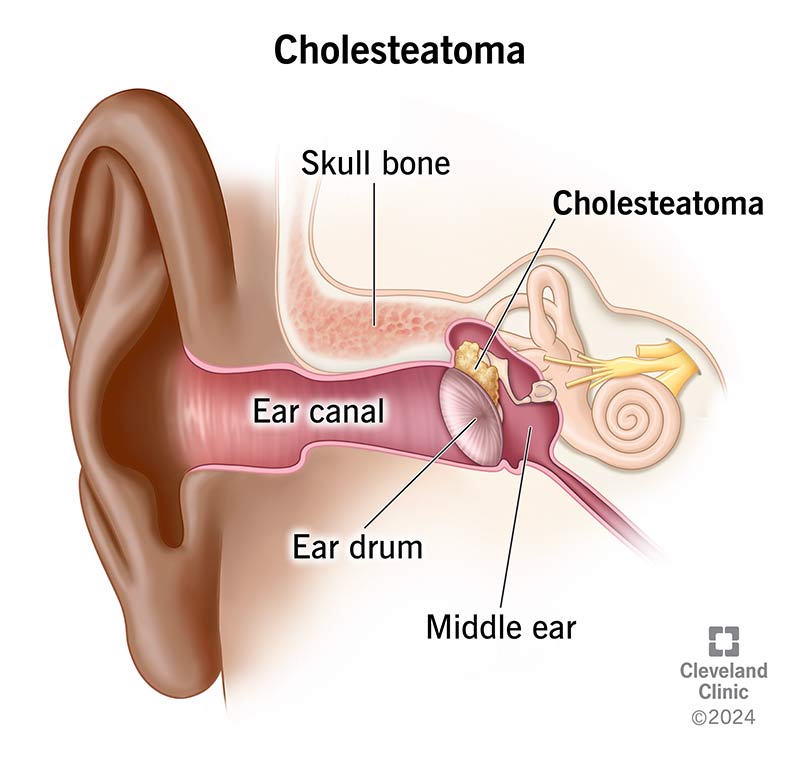
What is the mechanism by which we hear?
The ear is made up of three sections: the outer ear, the middle ear, and the inner ear. The middle ear is air-filled and located behind the eardrum (the tympanic membrane). The Eustachian tube, a tiny channel that runs from the rear of the nose up to the air, is where air enters.
The middle ear has three small bones (ossicles): the hammer (malleus), anvil (incus), and stirrup (stapes). The inner ear consists of the balance organ, which includes the semicircular canals, the utricle, and the saccule, as well as the cochlea.
The external ear receives sound waves that strike the eardrum. The eardrum vibrates in response to the sound waves. The sound vibrations travel from the eardrum to the ossicles. After that, the ossicles send the vibrations to the inner ear’s cochlea.
The cochlea transforms the vibrations into sound signals that are transmitted via a nerve from the ear to the brain, enabling us to hear.
The inner ear has two more structures known as the utricle and saccule, as well as the semicircular canals, all of which are filled with a fluid that shifts as we change positions. Minute hairs in the semicircular canals and the utricle and saccule detect the fluid’s movement and send signals via the ear nerve to the brain, which aids in maintaining balance and posture.
DISCLAIMER-Some patients go to net and directly take treatment from there which can lead to catastrophic consequences-Then- Many people ask then why to read all this text -the reason is that it helps you to understand the pathology better ,you can cooperate with treatment better ,your treating physician is already busy with his patients and he does not have sufficient time to explain you all the things right from ABCD ,so it is always better to have some knowledge of the disease /disorder you are suffering from.


