
Grisel’s Syndrome in Down Syndrome: Causes, Warning Signs & Treatment
By ENT Specialist – Dr. Sagar Rajkuwar, Nashik, Maharashtra, India
Clinic Website: www.entspecialistinnashik.com
Table of contents-
- Introduction
- What is Grisel’s syndrome?
- Gaining an Understanding of Cervical Instability and Down Syndrome
- The Connection Between Down Syndrome and Grisel’s Syndrome
- Symptoms and signs
- Diagnosis
- Treatment
- Prior to ENT surgery in individuals with Down syndrome, take precautions.
- Problems
- Prognosis
- Strategies for Prevention
- Conclusion
1)Introduction
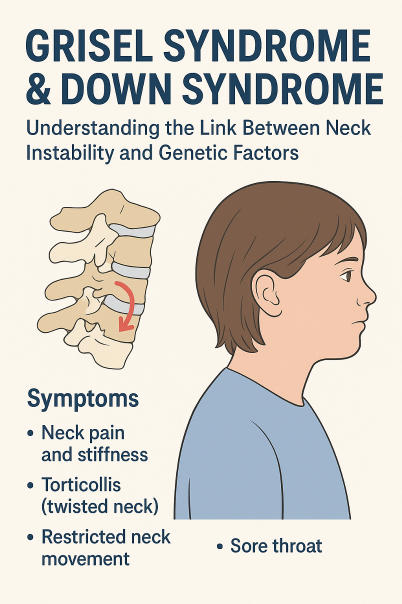
The uncommon but life-threatening disease known as Grisel’s syndrome occurs when the first two cervical vertebrae (C1 and C2) of the neck become misaligned as a result of non-traumatic atlantoaxial subluxation. Following ENT procedures like adenoidectomy or tonsillectomy, infections or inflammation in the head and neck area are frequent triggers.
Because of the intrinsic ligamentous laxity and cervical spine instability that are common in people with Down syndrome, the situation becomes more complicated when Grisel’s syndrome develops in these individuals. Knowing how these two disorders interact is essential for early identification, prevention, and successful surgical treatment.
The etiology, risk factors, signs, diagnosis, and treatment of Grisel’s syndrome are discussed in this piece, with a focus on when it occurs in conjunction with Down syndrome.
2)What is Grisel’s syndrome?
Inflammatory subluxation of the atlantoaxial joint (C1-C2) in the absence of trauma is known as Grisel’s syndrome. It frequently occurs following ENT surgery or upper respiratory tract infections, such as:
- removal of the adenoids
- Tonsil removal
- A mastoidectomy
- surgery on the sinuses
- infections of the throat or ear
Inflammatory hyperemia and spasm of the cervical muscles, which causes laxity in the atlantoaxial ligaments and ultimately results in rotatory subluxation of, are the main mechanisms. the atlas (C1) over the axis (C2).
Typical Reasons
- infections of the upper respiratory tract
- Sinusitis, otitis media, or pharyngitis
- Inflammation following ENT procedures
- Osteomyelitis of the cervical spine or tuberculosis (rare)
3)Gaining an Understanding of Cervical Instability and Down Syndrome
Trisomy 21, sometimes referred to as Down syndrome, is a genetic disease brought about by the presence of an additional chromosome 21. It is distinguished by intellectual impairment, hypotonia, and musculoskeletal problems such joint laxity and ligamentous weakness.
One of the primary orthopedic issues in Down syndrome is atlantoaxial instability (AAI), which is caused by excessive movement between the first and second cervical vertebrae. malformations of the odontoid process or loose ligaments.
Frequency of Atlantoaxial Instability in Down Syndrome
According to research:
- Radiological evidence of atlantoaxial instability is seen in around 15 to 20% of people with Down syndrome.
- About 1-2% of people may experience symptomatic instability, which can result in spinal cord compression.
Any inflammatory or surgical illness that affects the neck, like Grisel’s syndrome, might greatly raise the likelihood of spinal problems due to this pre-existing risk.
4)The Connection Between Down Syndrome and Grisel’s Syndrome
The ligaments in the cervical spine are inherently more flexible and less stable in youngsters and adults with Down syndrome. The ligamentous support around the atlantoaxial joint is further weakened when inflammation or infection occurs in the neighboring nasopharyngeal region (as in Grisel’s syndrome).
This combination results in a high-risk situation where even a minor illness, sore throat, or surgical operation might cause a hazardous neck subluxation.
Pathophysiology
- The atlantoaxial ligaments are connected to the nasopharyngeal or cervical tissues by venous or lymphatic pathways, through which inflammation can spread.
- This instability is exacerbated in individuals with Down syndrome by preexisting ligamentous laxity.
- Disalignment of the atlantoaxial joint causes subluxation or rotation of the atlas.
- If not identified early, this might lead to neck discomfort, torticollis, and, in some cases, spinal cord compression.
Down syndrome, therefore, functions as a predisposing factor that increases the risk and severity of Grisel’s syndrome.
5)Symptoms and signs
The signs of Grisel’s Syndrome
- Neck pain and stiffness
- Torticollis (twisted neck)
- Restricted neck movement
- head tilted to one side
- sore throat or low-grade fever
- A spasm of the muscles in the neck
- Neurologic symptoms are present in extreme situations, such as paralysis, tingling, and weakness.
DISCLAIMER-Some patients go to net and directly take treatment from there which can lead to catastrophic consequences-Then- Many people ask then why to read all this text -the reason is that it helps you to understand the pathology better ,you can cooperate with treatment better ,your treating physician is already busy with his patients and he does not have sufficient time to explain you all the things right from ABCD ,so it is always better to have some knowledge of the disease /disorder you are suffering from.
Other Issues in Down Syndrome Patients
Children with Down syndrome may experience the following challenges as a result of poor muscular tone and communication problems:
- Pain is not communicated effectively through speech.
- Exhibit unexplained irritability or a reluctance to turn the head.
- Symptoms may be mistaken for muscular torticollis or postoperative pain, resulting in a late diagnosis.
As a result, after any upper airway infection or ENT procedure, doctors and ENT surgeons must continue to have a high index of suspicion.
6)Diagnosis
In individuals with Down syndrome, early identification of Grisel’s syndrome is essential in order to prevent spinal cord damage.
Diagnostic Procedures
1.Clinical Assessment
- Check for neck stiffness, torticollis, and soreness.
- Look at any recent procedures or illnesses.
2.Radiological Photography
- X-ray of the cervical spine (open mouth perspective): May reveal asymmetry between C1 and C2.
- CT scan with 3D reconstruction: The best method for seeing the rotatory subluxation and the extent of the dislocation.
- MRI scan: assesses spinal cord compression, ligamentous damage, and soft tissue inflammation.
Classification of Hawkins and Fielding
The degree of atlantoaxial rotation and displacement determines the four types of Grisel’s syndrome:
- Type I: Rotation without any anterior movement.
- Type II: Rotation accompanied by an anterior shift of 3 to 5 mm.
- III type: Rotation with displacement greater than 5 mm.
- Type IV: Posterior displacement (uncommon and severe).
Down syndrome patients are more prone to advance to type II or III, requiring immediate treatment.
7)Treatment
Conservative treatment
during the initial phases (Type I and II), before any neurological symptoms appear:
- antibiotics to address the underlying infection.
- Muscle relaxants and anti-inflammatory medications to alleviate spasms.
- Utilizing a firm brace or soft collar to immobilize the neck for four to six weeks.
- bed rest with head support.
- Following the remission of acute pain, physiotherapy is administered.
Medical Intervention
In circumstances involving:
- Ongoing subluxation lasting more than six weeks.
- Cord compression or neurological deficits.
- Extreme malformation (Type III or IV).
Among the surgical choices are:
- Atlantoaxial fusion or stabilization with rods and screws.
- Posterior cervical fusion to stabilize the joint.
Due to the following reasons, surgery is often technically difficult for people with Down syndrome:
- Little skeletal constructions.
- Significant risk of anesthesia.
- Generalized hypotonia and inadequate healing.
As a result, the best course of action is still prevention and prompt, conservative treatment.
8)Prior to ENT surgery in individuals with Down syndrome, take precautions.
1. Preoperative Testing
Prior to any ENT procedure, such as adenoidectomy or tonsillectomy, all persons with Down syndrome should have cervical spine X-rays or MRI.
Before continuing, any indications of atlantoaxial instability should be discussed with an orthopedic or neurosurgeon.
2. During Surgery
Refrain from overextending the neck while intubating or positioning.
To avoid subluxation, use careful manipulation.
3. Follow-up Care Following Surgery
Watch out for torticollis, neck stiffness, or strange postures.
Report any neurological changes as soon as they occur.
9)Problems
Grissel’s syndrome can result in the following if left untreated:
- Neck deformity that persists over time
- Neurological deficit
- Spinal cord compression resulting in quadriplegia
- In extreme circumstances, respiratory failure may occur.
Because of the pre-existing instability, these complications can occur in individuals with Down syndrome even with modest inflammation; therefore, early diagnosis and immobilization are crucial.
10)Prognosis
Most patients recover completely without experiencing long-term neurological harm if they are properly diagnosed and treated right away.
Nevertheless, delayed diagnosis — particularly in Down syndrome — can lead to irreversible deformity or paralysis.
The outlook is contingent upon:
- The degree of subluxation
- When was the diagnosis made?
- Management appropriateness
To guarantee the maintenance of cervical stability, children with Down syndrome need ongoing follow-up and repeated imaging.
11)Strategies for Prevention
- Prompt care for infections of the ears, nose, and throat
- Refrain from moving your neck too much throughout operations
- Regular examination of Down syndrome patients for atlantoaxial instability
- Keeping an eye on the neck after surgery and providing support
- parent and caregiver education on the warning signs of torticollis
For important health related topics please click on our facebook page link given below or copy paste this link into google search –
https://www.facebook.com/positivemind.healthcare
For important health related videos please click on the link of our youtube channel given below or copy paste this link into google search-
http://www.youtube.com/@healthuseful8539
12)Conclusion
Due to their natural cervical spine laxity, people with Down syndrome are especially susceptible to the uncommon but potentially fatal condition known as Grisel’s syndrome. Pediatricians, ENT professionals, and anesthesiologists need to When treating or operating on such patients, maintain alertness.
The chance of atlantoaxial subluxation may be considerably decreased by ensuring preoperative screening, careful surgical handling, and postoperative monitoring.
Early identification and appropriate treatment are essential for protecting the quality of life for youngsters with Down syndrome as well as preventing neurological problems.
If any patient has any ENT -Ear nose throat problems and requires any , consultation ,online consultation ,or surgery in clinic of ENT specialist Doctor Dr Sagar Rajkuwar ,he may TAKE APPOINTMENT BY CLICKING ON THE LINK GIVEN BELOW-
www.entspecialistinnashik.com
Clinic address of ENT SPECIALIST doctor Dr Sagar Rajkuwar-
Prabha ENT clinic, plot no 345,Saigram colony, opposite Indoline furniture Ambad link road ,Ambad ,1 km from Pathardi phata Nashik ,422010 ,Maharashtra, India-Dr Sagar Rajkuwar (MS-ENT), Cell no- 7387590194 , 9892596635


